Difference between revisions of "Delayed Onset Muscle Soreness"
User:Fellrnr (User talk:Fellrnr | contribs) |
User:Fellrnr (User talk:Fellrnr | contribs) |
||
| (12 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
| − | Delayed Onset Muscle Soreness (DOMS) is a familiar experience to most people who exercise. It affects people who weight train and run particularly, and DOMS can produce anything from mild [[Muscle| muscle]] soreness to debilitating pain and weakness. DOMS is caused by eccentric stress, where the muscles working to resist lengthening, such as lowering a weight or absorbing the landing forces of running. [[Downhill Running | + | {{DISPLAYTITLE:Delayed Onset Muscle Soreness (DOMS) for Runners}} |
| + | DOMS is of critical importance for runners. Unlike many other types of exercise, running requires your muscles to extend under load, absorbing your weight as you land. This extension under load, called eccentric, is a prime cause of DOMS, and while the soreness is delayed, the accompanying weakness is immediate. This eccentric stress is why marathon runners are often hobbling around the day after a race. The good news is that a bout of DOMS inducing exercise provides protection against future DOMS, and so it's a critical part of training. This "Repeated Bout Effect" (RBE) is a core aspect of training, and by intentionally inducing DOMS you can prevent the soreness that occurs after long distance races. The less obvious, but more important benefit is that you also prevent some of the weakness that occurs towards the end of longer races. This is a key benefit to [[Downhill Running]] and especially the [[Treadmill Descent]]. I believe that incorporating Treadmill Descents into my training is the reason I've completed 100-mile races with little muscle soreness. | ||
| + | =Introduction = | ||
| + | Delayed Onset Muscle Soreness (DOMS) is a familiar experience to most people who exercise. It affects people who weight train and run particularly, and DOMS can produce anything from mild [[Muscle| muscle]] soreness to debilitating pain and weakness. DOMS is caused by eccentric stress, where the muscles working to resist lengthening, such as lowering a weight or absorbing the landing forces of running. [[Downhill Running]] is a particular source of eccentric stress. DOMS not only produces delayed soreness, but immediate weakness that generally lasts a similar length of time. DOMS also produces swelling, tense muscles, reduced coordination and a limited range of motion. A key benefit of DOMS inducing exercise is that a bout of DOMS can give protection against similar future exercise, and the protection lasts for months. This Repeated Bout Effect (RBE) is a critical part of endurance training. Running with the correct [[Cadence]] can help prevent DOMS, and [[Nutrient Timing| taking protein after DOMS inducing exercise]] is one of the best treatments, though [[Why compression clothes| compression clothing]], [[caffeine]] and [[massage]] can also help. It seems that [[Vitamin C]] may be critical to the RBE. | ||
=What is DOMS?= | =What is DOMS?= | ||
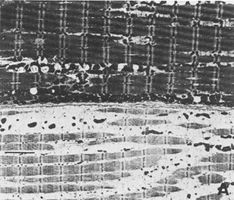
| − | The soreness of DOMS generally peaks between 24 and 72 hours after unusual or severe exercise, though soreness may occur sooner after running<ref name="Vickers2001"/>. DOMS is particularly related to eccentric exercise, which is where the muscle works to resist becoming longer, rather than working to contract. When | + | The soreness of DOMS generally peaks between 24 and 72 hours after unusual or severe exercise, though soreness may occur sooner after running<ref name="Vickers2001"/>. DOMS is particularly related to eccentric exercise, which is where the muscle works to resist becoming longer, rather than working to contract. When your muscles absorb the impact of running, this is eccentric exercise, and [[Downhill Running]] is more eccentric than flat or uphill running. The images below show the damage that occurs from eccentric exercise<ref name="FeassonStockholm2002"/> and marathon running<ref name="Warhol-1985"/>: |
<gallery widths=300px heights=200px caption="Muscle damage from eccentric exercise (downhill running)"> | <gallery widths=300px heights=200px caption="Muscle damage from eccentric exercise (downhill running)"> | ||
File:EccentricA.JPG|Muscle before downhill running | File:EccentricA.JPG|Muscle before downhill running | ||
| Line 23: | Line 26: | ||
* DOMS also reduces the strength of the effected muscles, and this can be quite dramatic in extreme cases. | * DOMS also reduces the strength of the effected muscles, and this can be quite dramatic in extreme cases. | ||
* Often a muscle with DOMS is hard to the touch, even when it's as relaxed as possible. A healthy muscle should only be firm when it's contracted. | * Often a muscle with DOMS is hard to the touch, even when it's as relaxed as possible. A healthy muscle should only be firm when it's contracted. | ||
| + | ==DOMS Scale== | ||
| + | This is a simplistic scale that I use to evaluate how bad my DOMS symptoms are. This is focused on DOMS of the quads, the most common areas noticed in runners. | ||
| + | {| class="wikitable" style="margin-left: auto; margin-right: auto; border: none;" | ||
| + | ! DOMS Scale | ||
| + | ! Stair Test | ||
| + | |- | ||
| + | | 0 | ||
| + | | You can walk down stairs without discomfort. | ||
| + | |- | ||
| + | | 1 | ||
| + | | You can walk down stairs with some pain, but there's no need to hold on to the handrail. | ||
| + | |- | ||
| + | | 2 | ||
| + | | You can walk down stairs with some pain, but you only need to hold on to the handrail for balance. | ||
| + | |- | ||
| + | | 3 | ||
| + | | You need to put some of your weight on the handrail to descend stairs. | ||
| + | |- | ||
| + | | 4 | ||
| + | | You need to put nearly all of your weight on the handrail to descend stairs. | ||
| + | |- | ||
| + | | 5 | ||
| + | | Your quads cannot lower any weight and descending stairs it tricky. Descending stairs involves standing opposite the handrail and locking the leg that is opposite the handrail. Your body is then tilted towards the handrail, using your arms to lower your weight. The leg nearest the handrail is locked straight and once your body is lowered, it takes the weight. Repeat for each step. (Or avoid stairs.) | ||
| + | |} | ||
| + | ==Likert Scale Muscle Soreness== | ||
| + | There is a more general scale of muscle soreness that applies to all muscles, but is not focused on DOMS<ref name="Vickers2001"/><ref name="Impellizzeri-2007"/>. | ||
| + | {| class="wikitable" style="margin-left: auto; margin-right: auto; border: none;" | ||
| + | ! Scale | ||
| + | ! Description | ||
| + | |- | ||
| + | | 0 | ||
| + | | An absence of soreness | ||
| + | |- | ||
| + | | 1 | ||
| + | | A light pain felt only when touched / a vague ache | ||
| + | |- | ||
| + | | 2 | ||
| + | | A moderate pain felt only when touched / a slight persistent pain | ||
| + | |- | ||
| + | | 3 | ||
| + | | A light pain when walking up or down stairs | ||
| + | |- | ||
| + | | 4 | ||
| + | | A light pain when walking on a flat surface / painful | ||
| + | |- | ||
| + | | 5 | ||
| + | | A moderate pain, stiffness or weakness when walking / very painful | ||
| + | |- | ||
| + | | 6 | ||
| + | | A severe pain that limits my ability to move | ||
| + | |} | ||
=What are the symptoms of DOMS?= | =What are the symptoms of DOMS?= | ||
| − | The soreness of DOMS is different to other forms of muscle soreness. With DOMS, large areas of the muscle are tender to the touch and painful when the muscle is used. With other forms of muscle soreness the area of tenderness is usually more localized and the pain of massage is sometimes described as a 'good pain'. The pain of DOMS will normally lessen with light exercise such as walking, which is often described as 'loosening' up. In addition, there are other symptoms, such as: | + | The soreness of DOMS is different to other forms of muscle soreness. With DOMS, large areas of the muscle are tender to the touch and painful when the muscle is used. With other forms of muscle soreness the area of tenderness is usually more localized and the pain of massage is sometimes described as a 'good pain'. The pain of DOMS will normally lessen with light exercise such as walking, which is often described as 'loosening' up. However, the soreness of DOMS is not the best indicator of the muscle damage, and similar levels of soreness can result from differing levels of muscle damage<ref name="NosakaNewton2002"/>. In addition, there are other symptoms, such as: |
* Reduction in strength<ref name="Saxton-1995"/><ref name="domsiso"/><ref name="Gulick-1996"/><ref name="Paddon-Jones-1997"/>, typically 30-60%<ref name="Baldwin Lanier-2003"/>. (Note that the reduction in strength starts immediately following the damaging exercise and increases over the next 24-48 hours<ref name="Cheung-2003"/>. The initial reduction in strength can be as much as 40%<ref name="Baldwin Lanier-2003"/>.) | * Reduction in strength<ref name="Saxton-1995"/><ref name="domsiso"/><ref name="Gulick-1996"/><ref name="Paddon-Jones-1997"/>, typically 30-60%<ref name="Baldwin Lanier-2003"/>. (Note that the reduction in strength starts immediately following the damaging exercise and increases over the next 24-48 hours<ref name="Cheung-2003"/>. The initial reduction in strength can be as much as 40%<ref name="Baldwin Lanier-2003"/>.) | ||
| + | * Muscle tenderness. DOMS makes the muscles tender to the touch, and the pain associated with pressure differs between DOMS and normal muscle soreness. With DOMS, the pain is extremely unpleasant and can be nauseating, where normal muscle soreness can be painful, but the pain has a sense of relief and is sometimes call a "good pain." The muscle tenderness can be measured from the "Pressure-Pain Threshold", where pressure is increased until the subject feels pain rather than pressure<ref name="Pearcey-2015"/>. | ||
* Increased passive muscle tension<ref name="Howatson-2008"/>. A muscle suffering from DOMS will often be hard to the touch, even when relaxed as much as possible. | * Increased passive muscle tension<ref name="Howatson-2008"/>. A muscle suffering from DOMS will often be hard to the touch, even when relaxed as much as possible. | ||
* Swelling of the muscle<ref name="Howatson-2008"/>, which can be seen as a lack of muscle definition in lean individuals. | * Swelling of the muscle<ref name="Howatson-2008"/>, which can be seen as a lack of muscle definition in lean individuals. | ||
| Line 34: | Line 89: | ||
* Impaired [[Glycogen]] repletion<ref name="Smith-1992"/><ref name="Braun-2003"/>, though higher carbohydrate intake partly offsets the reduction<ref name="Costill-1990"/>. There is some evidence that Glycogen levels continue to drop after DOMS inducing exercise<ref name="Zehnder-2004"/><ref name="Widrick-1992"/>, and the deficiency in glycogen lasts for over 72 hours<ref name="Widrick-1992"/>. | * Impaired [[Glycogen]] repletion<ref name="Smith-1992"/><ref name="Braun-2003"/>, though higher carbohydrate intake partly offsets the reduction<ref name="Costill-1990"/>. There is some evidence that Glycogen levels continue to drop after DOMS inducing exercise<ref name="Zehnder-2004"/><ref name="Widrick-1992"/>, and the deficiency in glycogen lasts for over 72 hours<ref name="Widrick-1992"/>. | ||
* There are some studies that indicate there are possible changes in muscle fiber recruitment patterns<ref name="Miles-1997"/><ref name="Zhou-1998"/><ref name="Zhou-1996"/>. | * There are some studies that indicate there are possible changes in muscle fiber recruitment patterns<ref name="Miles-1997"/><ref name="Zhou-1998"/><ref name="Zhou-1996"/>. | ||
| + | =How long does DOMS last?= | ||
| + | It seems likely that exercise characteristics (duration, intensity, etc.) will change the time to recovery<ref name="Vickers-2001"/><ref name="Paschalis-2005"/>. The soreness generally peaks between 24-72 hours after the damaging exercise, but will last at least 4 days<ref name="Paschalis-2005"/>. My personal experience is that DOMS can last for over a week, and I prefer to avoid [[Downhill Running]] in the two weeks before a race, though sometimes I will include it as close as 10 days beforehand. | ||
| + | =The effect of steepness on DOMS= | ||
| + | I have found that steeper descents produce disproportionately severe DOMS. This might be due to the angle of the knee, as most<ref name="Jones-1989"/><ref name="Child-1998"/> (but not all<ref name="Paschalis-2005"/>) studies indicate that the longer a muscle is when being stressed, the greater the DOMS. This effect is most noticeable when using a [[Treadmill]] for [[Downhill Running]], as small changes in angle can produce a big difference in DOMS. | ||
=How to prevent or treat DOMS?= | =How to prevent or treat DOMS?= | ||
There are various approaches to preventing or treating DOMS. The table below is a summary of the approaches showing how likely the strategy is to prevent or treat DOMS combined with the possible significant downsides. At the top are those that are likely to help and have no downsides, then those that have no effects or downsides, then those with little benefit and significant downsides. | There are various approaches to preventing or treating DOMS. The table below is a summary of the approaches showing how likely the strategy is to prevent or treat DOMS combined with the possible significant downsides. At the top are those that are likely to help and have no downsides, then those that have no effects or downsides, then those with little benefit and significant downsides. | ||
| − | {| class="wikitable" | + | {| class="wikitable" style="margin-left: auto; margin-right: auto; border: none;" |
| − | ! Strategy | + | ! '''Strategy ''' |
| − | ! Timing | + | ! '''Timing ''' |
| − | ! Soreness | + | ! '''Soreness ''' |
| − | ! Weakness | + | ! '''Weakness ''' |
| − | ! Downsides | + | ! '''Downsides ''' |
|- | |- | ||
| − | | Repeated Bout Effect | + | | Repeated Bout Effect |
| − | | Before (days to months) | + | | Before (days to months) |
| − | | Strong evidence of reduced soreness | + | | Strong evidence of reduced soreness |
| − | | Some evidence of reduced weakness | + | | Some evidence of reduced weakness |
| − | | None | + | | None |
|- | |- | ||
| [[Nutrient Timing| Carbohydrate and/or protein]] | | [[Nutrient Timing| Carbohydrate and/or protein]] | ||
| − | | After | + | | After |
| − | | Some evidence of reduced soreness | + | | Some evidence of reduced soreness |
| − | | Strong evidence of reduced weakness | + | | Strong evidence of reduced weakness |
| − | | None | + | | None |
|- | |- | ||
| [[Cadence]] | | [[Cadence]] | ||
| − | | During | + | | During |
| − | | Some evidence of reduced soreness | + | | Some evidence of reduced soreness |
| − | | Some evidence of reduced soreness | + | | Some evidence of reduced soreness |
| − | | None | + | | None |
|- | |- | ||
| [[Why compression clothes| Compression Clothing]] | | [[Why compression clothes| Compression Clothing]] | ||
| − | | After | + | | After |
| − | | Some evidence of reduced soreness | + | | Some evidence of reduced soreness |
| − | | Some evidence of reduced weakness | + | | Some evidence of reduced weakness |
| − | | None | + | | None |
|- | |- | ||
| [[Caffeine]] | | [[Caffeine]] | ||
| − | | After | + | | After |
| Some evidence of reduced soreness | | Some evidence of reduced soreness | ||
| − | | Some evidence of reduced weakness | + | | Some evidence of reduced weakness |
| − | | None<sup>a</sup> | + | | None<sup>a</sup> |
|- | |- | ||
| [[Massage]] | | [[Massage]] | ||
| − | | After | + | | After |
| − | | Some evidence of reduced soreness | + | | Some evidence of reduced soreness |
| − | | | + | | Some evidence of reduced weakness |
| − | | None | + | | None |
|- | |- | ||
| [[Warmup]] | | [[Warmup]] | ||
| − | | Immediately before | + | | Immediately before |
| − | | Some evidence of reduced soreness | + | | Some evidence of reduced soreness |
| − | | No benefit | + | | No benefit |
| − | | None | + | | None |
|- | |- | ||
| Light Exercise | | Light Exercise | ||
| − | | After | + | | After |
| Transient pain reduction | | Transient pain reduction | ||
| − | | No benefit | + | | No benefit |
| − | | None<sup>c</sup> | + | | None<sup>c</sup> |
|- | |- | ||
| − | | TENS | + | | TENS |
| − | | After | + | | After |
| Transient pain reduction | | Transient pain reduction | ||
| − | | No benefit | + | | No benefit |
| − | | None | + | | None |
|- | |- | ||
| [[Cryotherapy| Icing]] | | [[Cryotherapy| Icing]] | ||
| − | | After | + | | After |
| − | | No benefit | + | | No benefit |
| − | | No benefit | + | | No benefit |
| − | | None<sup>b</sup> | + | | None<sup>b</sup> |
|- | |- | ||
| − | | Antioxidents | + | | Antioxidents |
| − | | Before and/or After | + | | Before and/or After |
| − | | Mixed evidence | + | | Mixed evidence |
| − | | Mixed evidence | + | | Mixed evidence |
| Conflicting evidence of reduced [[Endurance Adaptations]] | | Conflicting evidence of reduced [[Endurance Adaptations]] | ||
|- | |- | ||
| [[Stretching]] | | [[Stretching]] | ||
| − | | Before and/or After | + | | Before and/or After |
| − | | No benefit | + | | No benefit |
| − | | No benefit | + | | No benefit |
| − | | | + | | # [[Stretching]]temporarily weakens muscles |
| − | + | # Can induce DOMS | |
| − | + | # Can lead to injury | |
| − | |||
|- | |- | ||
| [[NSAIDs and Running| NSAIDs]] | | [[NSAIDs and Running| NSAIDs]] | ||
| − | | Before and/or After | + | | Before and/or After |
| − | | Most evidence indicates no benefit | + | | Most evidence indicates no benefit |
| − | | Most evidence indicates no benefit | + | | Most evidence indicates no benefit |
| − | | Can impair recovery | + | | Can impair recovery |
|} | |} | ||
Notes | Notes | ||
| Line 131: | Line 189: | ||
The DOMS that follows an initial bout of eccentric exercise is much less on subsequent similar bouts. This is often called the Repeated Bout Effect (RBE)<ref name="Howatson-2008"/><ref name="Cheung-2003"/>. The initial bout does not have to cause significant soreness or damage<ref name="Clarkson-1987"/>. As few as 2-10 maximal eccentric repetitions can protect against a subsequent larger bout (24-50), but the initial bout must be close to maximal effort<ref name="Brown-1997"/>. By contrast, eight weeks of training with 50% of the maximal eccentric load did not provide protection against a subsequent maximal bout<ref name="Nosaka-2002"/>. There is some cross-over of protection between different forms of exercise. For instance, eccentric weight training protects against soreness and weakness in subsequent downhill running<ref name="Eston-1996"/>. The protection from the RBE is long lived. One study showed that while the initial weakness was not reduced by the RBE, the recovery of strength was much faster for up to 9 months, and soreness was less for up to 6 months<ref name="Nosaka-2001"/>. Another study showed that 30 minutes of downhill running provides protection for between 6 and 9 weeks<ref name="Byrnes-1985"/>. There is evidence that the RBE may rapidly start to provide protection from soreness and weakness<ref name="Mair-1995"/>, within 5 days<ref name="Ebbeling-1989"/>, and possibly within 24 hours<ref name="Chen-2001"/>. One study<ref name="Brockett-2001"/> demonstrated a change in the length-tension curve of DOMS trained muscles. As shown on the chart below, 7 days after a bout of DOMS inducing exercise the hamstring is able to generate more force and generate it at a greater angle. | The DOMS that follows an initial bout of eccentric exercise is much less on subsequent similar bouts. This is often called the Repeated Bout Effect (RBE)<ref name="Howatson-2008"/><ref name="Cheung-2003"/>. The initial bout does not have to cause significant soreness or damage<ref name="Clarkson-1987"/>. As few as 2-10 maximal eccentric repetitions can protect against a subsequent larger bout (24-50), but the initial bout must be close to maximal effort<ref name="Brown-1997"/>. By contrast, eight weeks of training with 50% of the maximal eccentric load did not provide protection against a subsequent maximal bout<ref name="Nosaka-2002"/>. There is some cross-over of protection between different forms of exercise. For instance, eccentric weight training protects against soreness and weakness in subsequent downhill running<ref name="Eston-1996"/>. The protection from the RBE is long lived. One study showed that while the initial weakness was not reduced by the RBE, the recovery of strength was much faster for up to 9 months, and soreness was less for up to 6 months<ref name="Nosaka-2001"/>. Another study showed that 30 minutes of downhill running provides protection for between 6 and 9 weeks<ref name="Byrnes-1985"/>. There is evidence that the RBE may rapidly start to provide protection from soreness and weakness<ref name="Mair-1995"/>, within 5 days<ref name="Ebbeling-1989"/>, and possibly within 24 hours<ref name="Chen-2001"/>. One study<ref name="Brockett-2001"/> demonstrated a change in the length-tension curve of DOMS trained muscles. As shown on the chart below, 7 days after a bout of DOMS inducing exercise the hamstring is able to generate more force and generate it at a greater angle. | ||
[[File:Length Tension Curve and DOMS.jpg|none|thumb|500px|A chart of a subject before and 7 days after DOMS inducing hamstring exercise. The chart shows the angle and the torque developed, indicating that after training the hamstrings are not only stronger, but are able to generate power at significantly longer length. This may be part of the underlying mechanism for the repeated bout effect.]] | [[File:Length Tension Curve and DOMS.jpg|none|thumb|500px|A chart of a subject before and 7 days after DOMS inducing hamstring exercise. The chart shows the angle and the torque developed, indicating that after training the hamstrings are not only stronger, but are able to generate power at significantly longer length. This may be part of the underlying mechanism for the repeated bout effect.]] | ||
| + | ===Repeated Bout and Vitamin C=== | ||
| + | I found a single study that looked at how the repeated bout effect changes with [[Vitamin C]]<ref name="HeHockemeyer2015"/>. As described below, most studies have found a small reduction in DOMS with Vitamin C. This 2014 study found that for the first bout, Vitamin C reduced the muscle soreness for the hamstrings, Quads, and Tibialis Anterior (shin), but the soreness of the glutes and calves were similar. However, for the second bout, not only was the soreness was reduced for the placebo, but it was further reduced with the Vitamin C. While this is just one study, it is intriguing with some profound implications. If the protective benefits of the repeated bout effect are dependent on nutritional (or other) factors, some runners may not get the benefit from their training. Personally, I've been taking ~1g/day of Vitamin C for many years due to [[Epidermolysis Bullosa| skin condition]]. However, the evidence that Vitamin C impairs the adaptation to exercise caused me to take a break for about 15 months. During that break from Vitamin C, I found my ability to perform downhill running was quite impaired, and I didn't seem to be able to build up resistance from the repeated bout effect. | ||
| + | [[File:Does Combined Antioxidant Vitamin Supplementation Blunt Repeated Bout Effect.jpg|center|thumb|500px|]] | ||
==Carbohydrate and Protein== | ==Carbohydrate and Protein== | ||
{{Main| Nutrient Timing}} | {{Main| Nutrient Timing}} | ||
| Line 152: | Line 213: | ||
==Compression Clothing == | ==Compression Clothing == | ||
{{Main| Why compression clothes}} | {{Main| Why compression clothes}} | ||
| − | Studies show that wearing [[Why compression clothes| Graduated Compression Clothing]] during the days after DOMS inducing exercise mitigates the soreness<ref name="DaviesThompson2009"/><ref name="Kraemer-2001"/><ref name="Kraemer-2001b"/><ref name="KraemerFlanagan2010"/><ref name="Jakeman-2010"/><ref name="Davies-2009"/><ref name="DuffieldPortus2007"/> and weakness<ref name="Kraemer-2001"/><ref name="KraemerFlanagan2010"/><ref name="Jakeman-2010"/> of DOMS. Relatively few studies showed no benefit from compression clothing<ref name="CarlingFrancis1995"/><ref name="Pearce-2009"/>. However, the results of compression clothing are likely to vary with the particular garment, how well it fits and therefore the pressure that is provided<ref name="MacRae-2011"/>. | + | Studies show that wearing [[Why compression clothes| Graduated Compression Clothing]] during the days after DOMS inducing exercise mitigates the soreness<ref name="DaviesThompson2009"/><ref name="Kraemer-2001"/><ref name="Kraemer-2001b"/><ref name="KraemerFlanagan2010"/><ref name="Jakeman-2010"/><ref name="Davies-2009"/><ref name="DuffieldPortus2007"/> and weakness<ref name="Kraemer-2001"/><ref name="KraemerFlanagan2010"/><ref name="Jakeman-2010"/> of DOMS. Relatively few studies showed no benefit from compression clothing<ref name="CarlingFrancis1995"/><ref name="Pearce-2009"/>. However, the results of compression clothing are likely to vary with the particular garment, how well it fits and therefore the pressure that is provided<ref name="MacRae-2011"/>. I found one studies that looked at the effect of wearing compression clothing during DOMS inducing exercise on the subsequent recovery<ref name="McDonnellCooper2018"/>. This study used either or both graduated or uniform compression socks on hiking, a trail run, or calf exercise, with the socks also worn for the following four days. Graduated socks reduced DOMS pain on the hike compared with no compression, the only test with no compression as a control. The uniform compression reduced the pain compared with graduated on the run, and there was no difference between them on the calf exercise. This suggests to me that uniform compression might be better than graduated, or at least, it might not be worth paying extra for graduated compression. |
==Caffeine== | ==Caffeine== | ||
{{Main| Caffeine}} | {{Main| Caffeine}} | ||
| Line 158: | Line 219: | ||
==Massage== | ==Massage== | ||
{{Main| Massage}} | {{Main| Massage}} | ||
| − | [[Massage]] is widely used to prevent and treat injuries. Most meta-analysis suggest that post-exercise massage helps with the soreness of DOMS<ref name="Ernst-1998"/><ref name="Moraska-2005"/>, though the mechanisms are unclear<ref name="Tiidus-1997"/>. Studies that give massage 2-3 hours after DOMS inducing exercise showed reduced soreness<ref name="Smith-1994"/><ref name="Zainuddin-2005"/><ref name="Hilbert2003"/>, but not weakness<ref name="Zainuddin-2005"/><ref name="Hilbert2003"/>. One study that gave massage 2 days after exercise that resulted in reduced soreness and improved muscle function<ref name="MancinelliDavis2006"/>, but other studies that use massage 24 hours or more after exercise showed no benefit<ref name="Hart-"/><ref name="Dawson-2004"/>. Therefore it seems likely that the timing of the massage is important, though other factors, such as the style of massage and the extent of the DOMS may also change the outcome. | + | [[Massage]] is widely used to prevent and treat injuries. Most meta-analysis suggest that post-exercise massage helps with the soreness of DOMS<ref name="Ernst-1998"/><ref name="Moraska-2005"/>, though the mechanisms are unclear<ref name="Tiidus-1997"/>. Studies that give massage 2-3 hours after DOMS inducing exercise showed reduced soreness<ref name="Smith-1994"/><ref name="Zainuddin-2005"/><ref name="Hilbert2003"/>, but not weakness<ref name="Zainuddin-2005"/><ref name="Hilbert2003"/>. One study that gave massage 2 days after exercise that resulted in reduced soreness and improved muscle function<ref name="MancinelliDavis2006"/>, but other studies that use massage 24 hours or more after exercise showed no benefit<ref name="Hart-"/><ref name="Dawson-2004"/>. A study that used 20 minutes of foam rolling immediately following the DOMS inducing exercise, then again at 24 and 48 hours showed a significant improvement in both pain and muscular performance<ref name="Pearcey-2015"/>. Therefore it seems likely that the timing of the massage is important, though other factors, such as the style of massage and the extent of the DOMS may also change the outcome. My personal experience suggests that massage immediately after the exercise is more effective than when the massage is delayed. (All too often, the muscles are too painful under pressure to allow any form of massage.) |
==Warmup== | ==Warmup== | ||
{{Main| Warmup}} | {{Main| Warmup}} | ||
Performing a [[Warmup]] before exercise may help reduce DOMS pain<ref name="Law-2007"/><ref name="RahnamaRahmani-Nia2005"/>, but not all studies support this<ref name="Evans-2002"/>. | Performing a [[Warmup]] before exercise may help reduce DOMS pain<ref name="Law-2007"/><ref name="RahnamaRahmani-Nia2005"/>, but not all studies support this<ref name="Evans-2002"/>. | ||
==Light Exercise== | ==Light Exercise== | ||
| − | Light training in the days following DOMS inducing exercise generally accepted to be one of the most effective ways of reducing muscle soreness, but unfortunately the reduction in pain is temporary<ref name="Armstrong-1984"/><ref name="Zainuddin-2006"/><ref name="Howatson-2008"/><ref name="Cheung-2003"/>. A study that looked at running 30 minutes/day after DOMS inducing downhill running shows that the extra exercise neither helped nor hindered with soreness, weakness or [[Running Economy]]<ref name="ChenNosaka2008"/>. (The study only looked at the 7 days following the downhill running, and it would be interesting to know if there are any longer term differences.) | + | Light training in the days following DOMS inducing exercise generally accepted to be one of the most effective ways of reducing muscle soreness, but unfortunately the reduction in pain is temporary<ref name="Armstrong-1984"/><ref name="Zainuddin-2006"/><ref name="Howatson-2008"/><ref name="Cheung-2003"/>. A study that looked at running 30 minutes/day after DOMS inducing downhill running shows that the extra exercise neither helped nor hindered with soreness, weakness or [[Running Economy]]<ref name="ChenNosaka2008"/>. (The study only looked at the 7 days following the downhill running, and it would be interesting to know if there are any longer-term differences.) One study used cycling at light (30%) or moderate (70%) immediately after DOMS inducing exercise<ref name="TufanoBrown2012"/>. The moderate intensity cycling prevented the loss of strength, and actually increased strength on days 3 and 4. There were no differences between the control and the light exercise, nor between any of the conditions for soreness. This is an interesting suggestion that higher intensity exercise might be beneficial, but the study has a number of flaws, including the use of predicted [[Maximum Heart Rate]] to set exercise intensity. |
==TENS== | ==TENS== | ||
TENS may reduce the soreness of DOMS<ref name="Denegar-1989"/>, but the effect seems to be transient<ref name="Denegar"/> and the effect is reduced if combined with icing<ref name="Denegar-1992"/>. Not all studies show any pain reduction<ref name="Bonacci-1997"/> and none show a reduction in the weakness. | TENS may reduce the soreness of DOMS<ref name="Denegar-1989"/>, but the effect seems to be transient<ref name="Denegar"/> and the effect is reduced if combined with icing<ref name="Denegar-1992"/>. Not all studies show any pain reduction<ref name="Bonacci-1997"/> and none show a reduction in the weakness. | ||
==Icing== | ==Icing== | ||
{{Main| Cryotherapy}} | {{Main| Cryotherapy}} | ||
| − | [[Cryotherapy| Icing]] does not help<ref name="Yackzan-"/><ref name="Shunsuke-2004"/><ref name="Gulick-17"/><ref name="Paddon-Jones-1997"/>, and can make DOMS worse<ref name="TsengLee2012"/><ref name="Isabell-1992"/>. Ice reduces pain slightly, but does not restore strength<ref name="Denegar-1992"/> | + | Sadly, [[Cryotherapy| Icing]] does not help with DOMS<ref name="Yackzan-"/><ref name="Shunsuke-2004"/><ref name="Gulick-17"/><ref name="Paddon-Jones-1997"/>, and can make DOMS worse<ref name="TsengLee2012"/><ref name="Isabell-1992"/>. Ice reduces pain slightly, but does not restore strength<ref name="Denegar-1992"/>. (In my experience, ice can be extremely effective at helping heal muscle tears and non-DOMS muscle injuries, but not DOMS.) |
| + | ==Protracted Heat== | ||
| + | One study looked at applying heat for 8 hours, either directly after DOMS inducing exercise or 24 hours later<ref name="PetrofskyBerk2017"/>. The study used "ThermaCare" chemically generated heat wraps, and I suspect the study was sponsored by the company. The 60 subjects underwent 5 minutes of squats to induce DOMS, then 20 were controls, 20 had immediate heat for 8 hours and the remainder had heat applied 24 hours after exercise. The immediate heat subjects had little reduction in strength over the follow three days, where the 24-hour delayed heat was no different from the controls. The strength drop was about 24% in controls/delayed-heat, which is a meaningful improvement. There was some reduction in pain over the first two days, with the immediate heat doing better than the delayed heat, which was slightly better than the controls. | ||
==Antioxidants - Vitamin C and E== | ==Antioxidants - Vitamin C and E== | ||
| − | The evidence for anti-oxidants is mixed, with some studies showing a benefit but not others. Note that one study below showed an impaired recovery with vitamin C supplementation. In addition, there is mixed evidence that vitamin C and/or vitamin E reduces [[Endurance Adaptations]] from exercise<ref name="Gomez-Cabrera-2008"/><ref name="RistowZarse2009"/><ref name="Strobel-2011"/> or they do not<ref name="Wadley-2010"/><ref name="Higashida-2011"/> <ref name="YfantiAkerstrom2009"/>. | + | The evidence for anti-oxidants is mixed, with some studies showing a benefit but not others. Note that one study below showed an impaired recovery with vitamin C supplementation. In addition, there is mixed evidence that vitamin C and/or vitamin E reduces [[Endurance Adaptations]] from exercise<ref name="Gomez-Cabrera-2008"/><ref name="RistowZarse2009"/><ref name="Strobel-2011"/> or they do not<ref name="Wadley-2010"/><ref name="Higashida-2011"/> <ref name="YfantiAkerstrom2009"/>. A 2019 systematic review of 50 studies covering 1,089 subjects concluded that there was moderate quality evidence that Vitamin C reduced DOMS at 48 and 96 hours, with lower quality evidence for 6 and 24 hours, but the reduction was quite small<ref name="RanchordasRogerson2018"/>. |
| − | {| class="wikitable" | + | {| class="wikitable" style="margin-left: auto; margin-right: auto; border: none;" |
! Vitamin C | ! Vitamin C | ||
! Vitamin E | ! Vitamin E | ||
| Line 229: | Line 292: | ||
==Stretching== | ==Stretching== | ||
{{Main| Stretching}} | {{Main| Stretching}} | ||
| − | [[Stretching]] before<ref name="High-1989"/><ref name="Johansson-1999"/> <ref name="Wessel-1994"/>, after <ref name="Johansson-1999"/><ref name="Buroker-1989"/><ref name="Herbert-2007"/>, or both before and after<ref name="Lund-1998"/> exercise does not help with DOMS. In fact, stretching alone can induce DOMS<ref name="Smith-1993"/>. | + | [[Stretching]] before<ref name="High-1989"/><ref name="Johansson-1999"/> <ref name="Wessel-1994"/>, after <ref name="Johansson-1999"/><ref name="Buroker-1989"/><ref name="Herbert-2007"/>, or both before and after<ref name="Lund-1998"/> exercise does not help with DOMS. In fact, stretching alone can induce DOMS<ref name="Smith-1993"/>. Both static and dynamic stretching are ineffective<ref name="XieFeng2018"/>. |
==NSAIDs== | ==NSAIDs== | ||
{{Main|NSAIDs and Running}} | {{Main|NSAIDs and Running}} | ||
| − | The most common NSAIDs (Ibuprofen, Acetaminophen | + | The most common NSAIDs (Ibuprofen, Acetaminophen/Paracetamol, and Aspirin) are unlikely to help with DOMS, but Naproxen may reduce the pain and weakness. If an NSAID is taken, it should probably be immediately after the damaging exercise rather than waiting until the soreness develops. It seems likely that taking an NSAID for DOMS will reduce the muscular growth that would normally occur as part of the recovery. In one disturbing study, rabbits treated with an NSAID (flurbiprofen) after DOMS inducing exercise initially recovered their strength after 3-7 days, but between days 7 and 28 days the rabbits became weaker while the untreated controls became stronger<ref name="Mishra-1995"/>. I have not included other animal studies, but this is the only one that looks at how NSAIDs impact the longer term recovery from DOMS. Studies of Turmeric, which acts as a selective COX-2 NSAID<ref name="RamsewakDeWitt2000"/>, are promising. Reduction in soreness is mixed, with some studies showing reduced soreness<ref name="Nicol-2015"/><ref name="Drobnic-2014"/> <ref name="NicolRowlands2015"/>, while others do not<ref name="McFarlinVenable2016"/><ref name="TanabeMaeda2015"/>. However, one study shoes reduced weakness and inflammation markers<ref name="TanabeMaeda2015"/> and an animal study showed less subsequent reduction in running performance in mice<ref name="Davis-2007"/>. Several studies showed reduced markers of damage<ref name="Kawanishi-2013"/><ref name="Davis-2007"/><ref name="TanabeMaeda2015"/><ref name="McFarlinVenable2016"/> <ref name="NicolRowlands2015"/>. However, Turmeric should be treated like any other medication as there are safety concerns; see [[NSAIDs_and_Running#Turmeric_as_an_NSAID| Turmeric as an NSAID]] for details. |
| − | {| class="wikitable" | + | {| class="wikitable" style="margin-left: auto; margin-right: auto; border: none;" |
! NSAID | ! NSAID | ||
! Soreness | ! Soreness | ||
| Line 282: | Line 345: | ||
| 1xNo Effect<ref name="Stone-2002"/> | | 1xNo Effect<ref name="Stone-2002"/> | ||
| | | | ||
| + | |- | ||
| + | | Turmeric | ||
| + | | 2xImproved<ref name="Nicol-2015"/><ref name="Drobnic-2014"/> | ||
| + | 2xNo Effect<ref name="McFarlinVenable2016"/><ref name="TanabeMaeda2015"/> | ||
| + | | 2xImproved<ref name="TanabeMaeda2015"/><ref name="Davis-2007"/> | ||
|} | |} | ||
| + | ==CBD Oil== | ||
| + | I have heard anecdotal suggestions that CBD oil may help with sleep after DOMS inducing exercise, but I've found no supporting research. Note that in 2018, World Anti-Doping Agency (WADA) removed CBD, from its 2018 prohibited substances list, but the legality of CBD is complex. | ||
| + | =Menstrual Cycle= | ||
| + | A study has shown that DOMS does not vary with menstrual cycle<ref name="ChaffinBerg2011"/>. | ||
=Mechanisms of DOMS= | =Mechanisms of DOMS= | ||
The underlying mechanism of DOMS is thought to consist of phases; the initial damage that occurs during the exercise and then secondary damage that occurs subsequently<ref name="Cheung-2003"/><ref name="Howatson-2008"/>: | The underlying mechanism of DOMS is thought to consist of phases; the initial damage that occurs during the exercise and then secondary damage that occurs subsequently<ref name="Cheung-2003"/><ref name="Howatson-2008"/>: | ||
| Line 296: | Line 368: | ||
** '''Increased passive muscle stiffness'''. In contrast, passive stiffness is when the muscles are relaxed. It is unclear if increased passive stiffness protects against eccentric damage or actually exacerbates it. | ** '''Increased passive muscle stiffness'''. In contrast, passive stiffness is when the muscles are relaxed. It is unclear if increased passive stiffness protects against eccentric damage or actually exacerbates it. | ||
* '''Cellular adaptation. '''A number of changes at the cellular level may provide protection against eccentric damage. | * '''Cellular adaptation. '''A number of changes at the cellular level may provide protection against eccentric damage. | ||
| − | ** '''Increased sarcomeres. '''The sarcomeres are part of the contracting mechanism of the muscles. The contraction of a muscle comes from parts of the sarcomere sliding over each other. One adaptation to eccentric exercise may be that the overlap in these sliding areas becomes larger. | + | ** '''Increased sarcomeres. '''The sarcomeres are part of the contracting mechanism of the muscles. The contraction of a muscle comes from parts of the sarcomere sliding over each other. One adaptation to eccentric exercise may be that the overlap in these sliding areas becomes larger. A study in rats suggests that the adaptation may include more sarcomeres in series, which produces a greater Range Of Motion and greater force at longer muscle lengths<ref name="Lynn-1998"/>. |
** '''Changed inflammation response. '''The delay in soreness is probably due to a delayed inflammatory response, so changes in that response could reduce the soreness. However, this would not reduce the immediate loss of strength. | ** '''Changed inflammation response. '''The delay in soreness is probably due to a delayed inflammatory response, so changes in that response could reduce the soreness. However, this would not reduce the immediate loss of strength. | ||
** '''Maintenance of Excitation-Contraction coupling'''. One reason for the loss of strength following eccentric exercise is that the nerve impulses (excitation) may result in less contraction. The decoupling could be due to lack of neural drive (perhaps due to pain), physical disruption of the contracting structures of the muscle, or a failure to activate those contracting structures. | ** '''Maintenance of Excitation-Contraction coupling'''. One reason for the loss of strength following eccentric exercise is that the nerve impulses (excitation) may result in less contraction. The decoupling could be due to lack of neural drive (perhaps due to pain), physical disruption of the contracting structures of the muscle, or a failure to activate those contracting structures. | ||
| Line 312: | Line 384: | ||
=References= | =References= | ||
<references> | <references> | ||
| + | <ref name="Paschalis-2005">V. Paschalis, Y. Koutedakis, AZ. Jamurtas, V. Mougios, V. Baltzopoulos, Equal volumes of high and low intensity of eccentric exercise in relation to muscle damage and performance., J Strength Cond Res, volume 19, issue 1, pages 184-8, Feb 2005, doi [http://dx.doi.org/10.1519/R-14763.1 10.1519/R-14763.1], PMID [http://www.ncbi.nlm.nih.gov/pubmed/15705032 15705032]</ref> | ||
| + | <ref name="ChaffinBerg2011">Morgan E. Chaffin, Kris E. Berg, Jessica R. Meendering, Tamra L. Llewellyn, Jeffrey A. French, Jeremy E. Davis, Interleukin-6 and Delayed Onset Muscle Soreness Do Not Vary During the Menstrual Cycle, Research Quarterly for Exercise and Sport, volume 82, issue 4, 2011, pages 693–701, ISSN [http://www.worldcat.org/issn/0270-1367 0270-1367], doi [http://dx.doi.org/10.1080/02701367.2011.10599806 10.1080/02701367.2011.10599806]</ref> | ||
<ref name="ChenNosaka2008">Trevor C. Chen, Kazunori Nosaka, Chia-Ching Wu, Effects of a 30-min running performed daily after downhill running on recovery of muscle function and running economy, Journal of Science and Medicine in Sport, volume 11, issue 3, 2008, pages 271–279, ISSN [http://www.worldcat.org/issn/14402440 14402440], doi [http://dx.doi.org/10.1016/j.jsams.2007.02.015 10.1016/j.jsams.2007.02.015]</ref> | <ref name="ChenNosaka2008">Trevor C. Chen, Kazunori Nosaka, Chia-Ching Wu, Effects of a 30-min running performed daily after downhill running on recovery of muscle function and running economy, Journal of Science and Medicine in Sport, volume 11, issue 3, 2008, pages 271–279, ISSN [http://www.worldcat.org/issn/14402440 14402440], doi [http://dx.doi.org/10.1016/j.jsams.2007.02.015 10.1016/j.jsams.2007.02.015]</ref> | ||
<ref name="Paschalis-2005"> V. Paschalis, Y. Koutedakis, V. Baltzopoulos, V. Mougios, AZ. Jamurtas, G. Giakas, Short vs. long length of rectus femoris during eccentric exercise in relation to muscle damage in healthy males., Clin Biomech (Bristol, Avon), volume 20, issue 6, pages 617-22, Jul 2005, doi [http://dx.doi.org/10.1016/j.clinbiomech.2005.02.011 10.1016/j.clinbiomech.2005.02.011], PMID [http://www.ncbi.nlm.nih.gov/pubmed/15927735 15927735]</ref> | <ref name="Paschalis-2005"> V. Paschalis, Y. Koutedakis, V. Baltzopoulos, V. Mougios, AZ. Jamurtas, G. Giakas, Short vs. long length of rectus femoris during eccentric exercise in relation to muscle damage in healthy males., Clin Biomech (Bristol, Avon), volume 20, issue 6, pages 617-22, Jul 2005, doi [http://dx.doi.org/10.1016/j.clinbiomech.2005.02.011 10.1016/j.clinbiomech.2005.02.011], PMID [http://www.ncbi.nlm.nih.gov/pubmed/15927735 15927735]</ref> | ||
| Line 391: | Line 465: | ||
<ref name="SmithGeorge1995">Lucille Smith, Robert George, Thomas Chenier, Michael McCammon, Joseph Houmard, Richard Israel, R. A. Hoppmann, Susan Smith, Do over-the-counter analgesics reduce delayed onset muscle soreness and serum creatine kinase values?, Research in Sports Medicine, volume 6, issue 2, 1995, pages 81–88, ISSN [http://www.worldcat.org/issn/1543-8627 1543-8627], doi [http://dx.doi.org/10.1080/15438629509512039 10.1080/15438629509512039]</ref> | <ref name="SmithGeorge1995">Lucille Smith, Robert George, Thomas Chenier, Michael McCammon, Joseph Houmard, Richard Israel, R. A. Hoppmann, Susan Smith, Do over-the-counter analgesics reduce delayed onset muscle soreness and serum creatine kinase values?, Research in Sports Medicine, volume 6, issue 2, 1995, pages 81–88, ISSN [http://www.worldcat.org/issn/1543-8627 1543-8627], doi [http://dx.doi.org/10.1080/15438629509512039 10.1080/15438629509512039]</ref> | ||
<ref name="Baldwin-2001"> AC. Baldwin, SW. Stevenson, GA. Dudley, Nonsteroidal anti-inflammatory therapy after eccentric exercise in healthy older individuals., J Gerontol A Biol Sci Med Sci, volume 56, issue 8, pages M510-3, Aug 2001, PMID [http://www.ncbi.nlm.nih.gov/pubmed/11487604 11487604]</ref> | <ref name="Baldwin-2001"> AC. Baldwin, SW. Stevenson, GA. Dudley, Nonsteroidal anti-inflammatory therapy after eccentric exercise in healthy older individuals., J Gerontol A Biol Sci Med Sci, volume 56, issue 8, pages M510-3, Aug 2001, PMID [http://www.ncbi.nlm.nih.gov/pubmed/11487604 11487604]</ref> | ||
| − | <ref name="pmid12580656">Tokmakidis SP, Kokkinidis EA, Smilios I, Douda H, The effects of ibuprofen on delayed muscle soreness and muscular performance after eccentric exercise., J Strength Cond Res, 2003, volume 17, issue 1, pages 53-9, PMID [http://www.ncbi.nlm.nih.gov/pubmed/12580656 12580656] </ref> | + | <ref name="pmid12580656">author Tokmakidis SP, Kokkinidis EA, Smilios I, Douda H, The effects of ibuprofen on delayed muscle soreness and muscular performance after eccentric exercise., J Strength Cond Res, 2003, volume 17, issue 1, pages 53-9, PMID [http://www.ncbi.nlm.nih.gov/pubmed/12580656 12580656] </ref> |
<ref name="Stone-2002"> MB. Stone, MA. Merrick, CD. Ingersoll, JE. Edwards, Preliminary comparison of bromelain and Ibuprofen for delayed onset muscle soreness management., Clin J Sport Med, volume 12, issue 6, pages 373-8, Nov 2002, PMID [http://www.ncbi.nlm.nih.gov/pubmed/12466693 12466693]</ref> | <ref name="Stone-2002"> MB. Stone, MA. Merrick, CD. Ingersoll, JE. Edwards, Preliminary comparison of bromelain and Ibuprofen for delayed onset muscle soreness management., Clin J Sport Med, volume 12, issue 6, pages 373-8, Nov 2002, PMID [http://www.ncbi.nlm.nih.gov/pubmed/12466693 12466693]</ref> | ||
<ref name="RahnamaRahmani-Nia2005">N Rahnama, F Rahmani-Nia, K Ebrahim, The isolated and combined effects of selected physical activity and ibuprofen on delayed-onset muscle soreness, Journal of Sports Sciences, volume 23, issue 8, 2005, pages 843–850, ISSN [http://www.worldcat.org/issn/0264-0414 0264-0414], doi [http://dx.doi.org/10.1080/02640410400021989 10.1080/02640410400021989]</ref> | <ref name="RahnamaRahmani-Nia2005">N Rahnama, F Rahmani-Nia, K Ebrahim, The isolated and combined effects of selected physical activity and ibuprofen on delayed-onset muscle soreness, Journal of Sports Sciences, volume 23, issue 8, 2005, pages 843–850, ISSN [http://www.worldcat.org/issn/0264-0414 0264-0414], doi [http://dx.doi.org/10.1080/02640410400021989 10.1080/02640410400021989]</ref> | ||
| Line 453: | Line 527: | ||
<ref name="Derrick-1998"> TR. Derrick, J. Hamill, GE. Caldwell, Energy absorption of impacts during running at various stride lengths., Med Sci Sports Exerc, volume 30, issue 1, pages 128-35, Jan 1998, PMID [http://www.ncbi.nlm.nih.gov/pubmed/9475654 9475654]</ref> | <ref name="Derrick-1998"> TR. Derrick, J. Hamill, GE. Caldwell, Energy absorption of impacts during running at various stride lengths., Med Sci Sports Exerc, volume 30, issue 1, pages 128-35, Jan 1998, PMID [http://www.ncbi.nlm.nih.gov/pubmed/9475654 9475654]</ref> | ||
<ref name="Clarke-1985"> TE. Clarke, LB. Cooper, CL. Hamill, DE. Clark, The effect of varied stride rate upon shank deceleration in running., J Sports Sci, volume 3, issue 1, pages 41-9, 1985, doi [http://dx.doi.org/10.1080/02640418508729731 10.1080/02640418508729731], PMID [http://www.ncbi.nlm.nih.gov/pubmed/4094019 4094019]</ref> | <ref name="Clarke-1985"> TE. Clarke, LB. Cooper, CL. Hamill, DE. Clark, The effect of varied stride rate upon shank deceleration in running., J Sports Sci, volume 3, issue 1, pages 41-9, 1985, doi [http://dx.doi.org/10.1080/02640418508729731 10.1080/02640418508729731], PMID [http://www.ncbi.nlm.nih.gov/pubmed/4094019 4094019]</ref> | ||
| + | <ref name="NosakaNewton2002">Kazunori Nosaka, Mike Newton, Paul Sacco, Delayed-onset muscle soreness does not reflect the magnitude of eccentric exercise-induced muscle damage, Scandinavian Journal of Medicine & Science in Sports, volume 12, issue 6, 2002, pages 337–346, ISSN [http://www.worldcat.org/issn/09057188 09057188], doi [http://dx.doi.org/10.1034/j.1600-0838.2002.10178.x 10.1034/j.1600-0838.2002.10178.x]</ref> | ||
| + | <ref name="Vickers-2001"> AJ. Vickers, Time course of muscle soreness following different types of exercise., BMC Musculoskelet Disord, volume 2, pages 5, 2001, PMID [http://www.ncbi.nlm.nih.gov/pubmed/11701094 11701094]</ref> | ||
| + | <ref name="Lynn-1998">R. Lynn, JA. Talbot, DL. Morgan, Differences in rat skeletal muscles after incline and decline running., J Appl Physiol (1985), volume 85, issue 1, pages 98-104, Jul 1998, PMID [http://www.ncbi.nlm.nih.gov/pubmed/9655761 9655761]</ref> | ||
| + | <ref name="Vickers2001">Andrew J Vickers, BMC Musculoskeletal Disorders, volume 2, issue 1, 2001, pages 5, ISSN [http://www.worldcat.org/issn/14712474 14712474], doi [http://dx.doi.org/10.1186/1471-2474-2-5 10.1186/1471-2474-2-5]</ref> | ||
| + | <ref name="Impellizzeri-2007">FM. Impellizzeri, NA. Maffiuletti, Convergent evidence for construct validity of a 7-point likert scale of lower limb muscle soreness., Clin J Sport Med, volume 17, issue 6, pages 494-6, Nov 2007, doi [http://dx.doi.org/10.1097/JSM.0b013e31815aed57 10.1097/JSM.0b013e31815aed57], PMID [http://www.ncbi.nlm.nih.gov/pubmed/17993794 17993794]</ref> | ||
| + | <ref name="Pearcey-2015">GE. Pearcey, DJ. Bradbury-Squires, JE. Kawamoto, EJ. Drinkwater, DG. Behm, DC. Button, Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures., J Athl Train, volume 50, issue 1, pages 5-13, Jan 2015, doi [http://dx.doi.org/10.4085/1062-6050-50.1.01 10.4085/1062-6050-50.1.01], PMID [http://www.ncbi.nlm.nih.gov/pubmed/25415413 25415413]</ref> | ||
| + | <ref name="RamsewakDeWitt2000">R.S. Ramsewak, D.L. DeWitt, M.G. Nair, Cytotoxicity, antioxidant and anti-inflammatory activities of Curcumins I–III from Curcuma longa, Phytomedicine, volume 7, issue 4, 2000, pages 303–308, ISSN [http://www.worldcat.org/issn/09447113 09447113], doi [http://dx.doi.org/10.1016/S0944-7113(00)80048-3 10.1016/S0944-7113(00)80048-3]</ref> | ||
| + | <ref name="Nicol-2015">LM. Nicol, DS. Rowlands, R. Fazakerly, J. Kellett, Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS)., Eur J Appl Physiol, volume 115, issue 8, pages 1769-77, Aug 2015, doi [http://dx.doi.org/10.1007/s00421-015-3152-6 10.1007/s00421-015-3152-6], PMID [http://www.ncbi.nlm.nih.gov/pubmed/25795285 25795285]</ref> | ||
| + | <ref name="Drobnic-2014">F. Drobnic, J. Riera, G. Appendino, S. Togni, F. Franceschi, X. Valle, A. Pons, J. Tur, Reduction of delayed onset muscle soreness by a novel curcumin delivery system (Meriva): a randomised, placebo-controlled trial., J Int Soc Sports Nutr, volume 11, pages 31, 2014, doi [http://dx.doi.org/10.1186/1550-2783-11-31 10.1186/1550-2783-11-31], PMID [http://www.ncbi.nlm.nih.gov/pubmed/24982601 24982601]</ref> | ||
| + | <ref name="McFarlinVenable2016">Brian K. McFarlin, Adam S. Venable, Andrea L. Henning, Jill N. Best Sampson, Kathryn Pennel, Jakob L. Vingren, David W. Hill, Reduced Inflammatory and Muscle Damage Biomarkers following Oral Supplementation with Bioavailable Curcumin, BBA Clinical, 2016, ISSN [http://www.worldcat.org/issn/22146474 22146474], doi [http://dx.doi.org/10.1016/j.bbacli.2016.02.003 10.1016/j.bbacli.2016.02.003]</ref> | ||
| + | <ref name="TanabeMaeda2015">Yoko Tanabe, Seiji Maeda, Nobuhiko Akazawa, Asako Zempo-Miyaki, Youngju Choi, Song-Gyu Ra, Atsushi Imaizumi, Yoshihiko Otsuka, Kazunori Nosaka, Attenuation of indirect markers of eccentric exercise-induced muscle damage by curcumin, European Journal of Applied Physiology, volume 115, issue 9, 2015, pages 1949–1957, ISSN [http://www.worldcat.org/issn/1439-6319 1439-6319], doi [http://dx.doi.org/10.1007/s00421-015-3170-4 10.1007/s00421-015-3170-4]</ref> | ||
| + | <ref name="Davis-2007">JM. Davis, EA. Murphy, MD. Carmichael, MR. Zielinski, CM. Groschwitz, AS. Brown, JD. Gangemi, A. Ghaffar, EP. Mayer, Curcumin effects on inflammation and performance recovery following eccentric exercise-induced muscle damage., Am J Physiol Regul Integr Comp Physiol, volume 292, issue 6, pages R2168-73, Jun 2007, doi [http://dx.doi.org/10.1152/ajpregu.00858.2006 10.1152/ajpregu.00858.2006], PMID [http://www.ncbi.nlm.nih.gov/pubmed/17332159 17332159]</ref> | ||
| + | <ref name="Kawanishi-2013">N. Kawanishi, K. Kato, M. Takahashi, T. Mizokami, Y. Otsuka, A. Imaizumi, D. Shiva, H. Yano, K. Suzuki, Curcumin attenuates oxidative stress following downhill running-induced muscle damage., Biochem Biophys Res Commun, volume 441, issue 3, pages 573-8, Nov 2013, doi [http://dx.doi.org/10.1016/j.bbrc.2013.10.119 10.1016/j.bbrc.2013.10.119], PMID [http://www.ncbi.nlm.nih.gov/pubmed/24184481 24184481]</ref> | ||
| + | <ref name="PetrofskyBerk2017">Jerrold Petrofsky, Lee Berk, Gurinder Bains, Iman Akef Khowailed, Haneul Lee, Michael Laymon, The Efficacy of Sustained Heat Treatment on Delayed-Onset Muscle Soreness, Clinical Journal of Sport Medicine, volume 27, issue 4, 2017, pages 329–337, ISSN [http://www.worldcat.org/issn/1050-642X 1050-642X], doi [http://dx.doi.org/10.1097/JSM.0000000000000375 10.1097/JSM.0000000000000375]</ref> | ||
| + | <ref name="XieFeng2018">Yanfei Xie, Beibei Feng, Kedi Chen, Lars L. Andersen, Phil Page, Yuling Wang, The Efficacy of Dynamic Contract-Relax Stretching on Delayed-Onset Muscle Soreness Among Healthy Individuals, Clinical Journal of Sport Medicine, volume 28, issue 1, 2018, pages 28–36, ISSN [http://www.worldcat.org/issn/1050-642X 1050-642X], doi [http://dx.doi.org/10.1097/JSM.0000000000000442 10.1097/JSM.0000000000000442]</ref> | ||
| + | <ref name="NicolRowlands2015">Lesley M. Nicol, David S. Rowlands, Ruth Fazakerly, John Kellett, Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS), European Journal of Applied Physiology, volume 115, issue 8, 2015, pages 1769–1777, ISSN [http://www.worldcat.org/issn/1439-6319 1439-6319], doi [http://dx.doi.org/10.1007/s00421-015-3152-6 10.1007/s00421-015-3152-6]</ref> | ||
| + | <ref name="McDonnellCooper2018">Adam C McDonnell, Diane Cooper, Tinkara Mlinar, Igor B Mekjavic, The effect of post-exercise application of either graduated or uniform compression socks on the mitigation of delayed onset muscle soreness, Textile Research Journal, 2018, pages 004051751878000, ISSN [http://www.worldcat.org/issn/0040-5175 0040-5175], doi [http://dx.doi.org/10.1177/0040517518780002 10.1177/0040517518780002]</ref> | ||
| + | <ref name="TufanoBrown2012">James J. Tufano, Lee E. Brown, Jared W. Coburn, Kavin K.W. Tsang, Vanessa L. Cazas, Joe W. LaPorta, Effect of Aerobic Recovery Intensity on Delayed-Onset Muscle Soreness and Strength, Journal of Strength and Conditioning Research, volume 26, issue 10, 2012, pages 2777–2782, ISSN [http://www.worldcat.org/issn/1064-8011 1064-8011], doi [http://dx.doi.org/10.1519/JSC.0b013e3182651c06 10.1519/JSC.0b013e3182651c06]</ref> | ||
| + | <ref name="RanchordasRogerson2018">Mayur K Ranchordas, David Rogerson, Hora Soltani, Joseph T Costello, Antioxidants for preventing and reducing muscle soreness after exercise: a Cochrane systematic review, British Journal of Sports Medicine, 2018, pages bjsports-2018-099599, ISSN [http://www.worldcat.org/issn/0306-3674 0306-3674], doi [http://dx.doi.org/10.1136/bjsports-2018-099599 10.1136/bjsports-2018-099599]</ref> | ||
| + | <ref name="HeHockemeyer2015">F. He, J. Hockemeyer, D. Sedlock, Does Combined Antioxidant Vitamin Supplementation Blunt Repeated Bout Effect?, International Journal of Sports Medicine, volume 36, issue 05, 2015, pages 407–413, ISSN [http://www.worldcat.org/issn/0172-4622 0172-4622], doi [http://dx.doi.org/10.1055/s-0034-1395630 10.1055/s-0034-1395630]</ref> | ||
</references> | </references> | ||
Revision as of 13:58, 6 January 2020
DOMS is of critical importance for runners. Unlike many other types of exercise, running requires your muscles to extend under load, absorbing your weight as you land. This extension under load, called eccentric, is a prime cause of DOMS, and while the soreness is delayed, the accompanying weakness is immediate. This eccentric stress is why marathon runners are often hobbling around the day after a race. The good news is that a bout of DOMS inducing exercise provides protection against future DOMS, and so it's a critical part of training. This "Repeated Bout Effect" (RBE) is a core aspect of training, and by intentionally inducing DOMS you can prevent the soreness that occurs after long distance races. The less obvious, but more important benefit is that you also prevent some of the weakness that occurs towards the end of longer races. This is a key benefit to Downhill Running and especially the Treadmill Descent. I believe that incorporating Treadmill Descents into my training is the reason I've completed 100-mile races with little muscle soreness.
Contents
- 1 Introduction
- 2 What is DOMS?
- 3 Why is DOMS important?
- 4 What does DOMS mean to you?
- 5 Determining if you have DOMS
- 6 What are the symptoms of DOMS?
- 7 How long does DOMS last?
- 8 The effect of steepness on DOMS
- 9 How to prevent or treat DOMS?
- 10 Menstrual Cycle
- 11 Mechanisms of DOMS
- 12 Limitations of the current scientific studies
- 13 See Also
- 14 References
1 Introduction
Delayed Onset Muscle Soreness (DOMS) is a familiar experience to most people who exercise. It affects people who weight train and run particularly, and DOMS can produce anything from mild muscle soreness to debilitating pain and weakness. DOMS is caused by eccentric stress, where the muscles working to resist lengthening, such as lowering a weight or absorbing the landing forces of running. Downhill Running is a particular source of eccentric stress. DOMS not only produces delayed soreness, but immediate weakness that generally lasts a similar length of time. DOMS also produces swelling, tense muscles, reduced coordination and a limited range of motion. A key benefit of DOMS inducing exercise is that a bout of DOMS can give protection against similar future exercise, and the protection lasts for months. This Repeated Bout Effect (RBE) is a critical part of endurance training. Running with the correct Cadence can help prevent DOMS, and taking protein after DOMS inducing exercise is one of the best treatments, though compression clothing, caffeine and massage can also help. It seems that Vitamin C may be critical to the RBE.
2 What is DOMS?
The soreness of DOMS generally peaks between 24 and 72 hours after unusual or severe exercise, though soreness may occur sooner after running[1]. DOMS is particularly related to eccentric exercise, which is where the muscle works to resist becoming longer, rather than working to contract. When your muscles absorb the impact of running, this is eccentric exercise, and Downhill Running is more eccentric than flat or uphill running. The images below show the damage that occurs from eccentric exercise[2] and marathon running[3]:
- Muscle damage from eccentric exercise (downhill running)
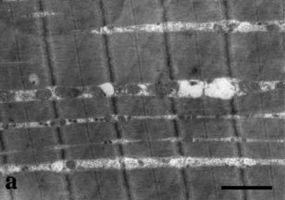
Muscle before downhill running
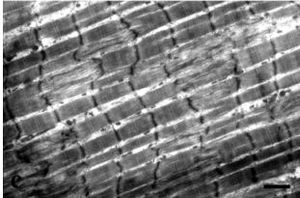
Immediately after downhill running. Notice the disruption to the dark bands (z-bands) that are part of the muscle structure showing there is immediate damage.
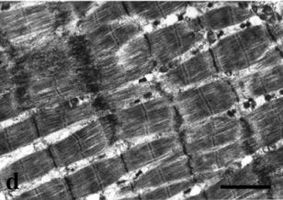
One day later, the damage and disruption is worse, indicated some continued breakdown.
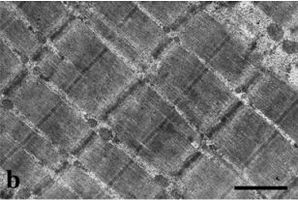
Muscle 14 days later, structurally recovered (other metrics do not return to pre-exercise levels at 14 days).




- Muscle damage after running a marathon
The selective pattern of damage, showing the normal upper fiber adjacent to the 'moth eaten' appearance of the damaged lower fiber.
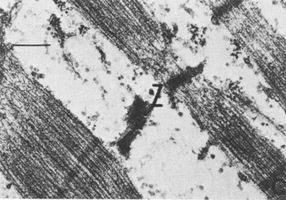
Here you can see extreme damage, with only the Z band of the fiber remaining (marked Z). Adjacent fibers show far less damage.


3 Why is DOMS important?
Because running involves a lot of eccentric stress, DOMS is common in runners, especially after Downhill Running. The pain that occurs 24-72 hours after exercise can prevent continued training. However, the biggest issue for long distance runners is that although the pain occurs 24-72 hours after exercise, the weakness peaks after 30 minutes [4]/>. If you've ever run a long, steep descent, you'll know the strange feeling of weak numbness that pervades your quads as the effect of the downhill builds up. The Boston Marathon or the latter part of Mount Mitchell Challenge have descents that cause this type of weakness. If you've felt a similar weakness in the latter stages of a marathon, this may not be Glycogen depletion creating 'the wall', but eccentric muscle damage that will later manifest itself as DOMS. It is suggested that this is the reason the Boston Marathon course is relatively slow, even though it is a net decent.
4 What does DOMS mean to you?
There is some good news in all of this. While excessive eccentric exercise can cause DOMS, doing some eccentric exercise causes the muscles to adapt and to be able to handle eccentric exercise without DOMS [5]. There are two ways then of protecting your muscles from DOMS in running; running greater distances, or running downhill. I believe that downhill running that is greatly underutilized in training regimes. Most hill training workouts focus on the uphill segment, and relegate the downhill to recovery. While uphill can produce some benefits, it is the downhill that can provide the greatest advantage. Adding hills into your workout can make you a much stronger runner, and have benefits even on flat race courses. Don't just use the downhill to recover from the uphill, but work on the downhill.
5 Determining if you have DOMS
It's not always obvious if you have DOMS or some other problem. Here are some simple checks that can help guide you:
- As the name suggests, DOMS normally occurs a day or two after the exercise, but this is not always the case.
- The soreness of DOMS eases off with light exercise, so if the pain gets less then it's probably DOMS but if it gets worse it's probably not. The lessoning of the pain should occur after a few minutes of light exercise, such as walking or gentle running.
- The soreness of DOMS is normally quite diffuse over a large area of the muscle and the soreness is close to the surface. Often the muscles are tender to the touch and Massage is too painful. That is different to something like a muscle tear which has a sharp, localized pain, or a Trigger Point that has a painful lump in the muscle.
- DOMS also reduces the strength of the effected muscles, and this can be quite dramatic in extreme cases.
- Often a muscle with DOMS is hard to the touch, even when it's as relaxed as possible. A healthy muscle should only be firm when it's contracted.
5.1 DOMS Scale
This is a simplistic scale that I use to evaluate how bad my DOMS symptoms are. This is focused on DOMS of the quads, the most common areas noticed in runners.
| DOMS Scale | Stair Test |
|---|---|
| 0 | You can walk down stairs without discomfort. |
| 1 | You can walk down stairs with some pain, but there's no need to hold on to the handrail. |
| 2 | You can walk down stairs with some pain, but you only need to hold on to the handrail for balance. |
| 3 | You need to put some of your weight on the handrail to descend stairs. |
| 4 | You need to put nearly all of your weight on the handrail to descend stairs. |
| 5 | Your quads cannot lower any weight and descending stairs it tricky. Descending stairs involves standing opposite the handrail and locking the leg that is opposite the handrail. Your body is then tilted towards the handrail, using your arms to lower your weight. The leg nearest the handrail is locked straight and once your body is lowered, it takes the weight. Repeat for each step. (Or avoid stairs.) |
5.2 Likert Scale Muscle Soreness
There is a more general scale of muscle soreness that applies to all muscles, but is not focused on DOMS[1][6].
| Scale | Description |
|---|---|
| 0 | An absence of soreness |
| 1 | A light pain felt only when touched / a vague ache |
| 2 | A moderate pain felt only when touched / a slight persistent pain |
| 3 | A light pain when walking up or down stairs |
| 4 | A light pain when walking on a flat surface / painful |
| 5 | A moderate pain, stiffness or weakness when walking / very painful |
| 6 | A severe pain that limits my ability to move |
6 What are the symptoms of DOMS?
The soreness of DOMS is different to other forms of muscle soreness. With DOMS, large areas of the muscle are tender to the touch and painful when the muscle is used. With other forms of muscle soreness the area of tenderness is usually more localized and the pain of massage is sometimes described as a 'good pain'. The pain of DOMS will normally lessen with light exercise such as walking, which is often described as 'loosening' up. However, the soreness of DOMS is not the best indicator of the muscle damage, and similar levels of soreness can result from differing levels of muscle damage[7]. In addition, there are other symptoms, such as:
- Reduction in strength[8][9][10][11], typically 30-60%[12]. (Note that the reduction in strength starts immediately following the damaging exercise and increases over the next 24-48 hours[13]. The initial reduction in strength can be as much as 40%[12].)
- Muscle tenderness. DOMS makes the muscles tender to the touch, and the pain associated with pressure differs between DOMS and normal muscle soreness. With DOMS, the pain is extremely unpleasant and can be nauseating, where normal muscle soreness can be painful, but the pain has a sense of relief and is sometimes call a "good pain." The muscle tenderness can be measured from the "Pressure-Pain Threshold", where pressure is increased until the subject feels pain rather than pressure[14].
- Increased passive muscle tension[15]. A muscle suffering from DOMS will often be hard to the touch, even when relaxed as much as possible.
- Swelling of the muscle[15], which can be seen as a lack of muscle definition in lean individuals.
- The perceptions of joint angle and force are impaired[8], which can result in reduced coordination and a sense of clumsiness.
- A reduction in the Range of Motion[8][9][10].
- Changes in running biomechanics, possibly as compensation for other changes[16]. For instance, the reduction in Range of Motion can result in a reduction in stride length.
- Decreased Running Economy[17][18].
- Impaired Glycogen repletion[17][18], though higher carbohydrate intake partly offsets the reduction[19]. There is some evidence that Glycogen levels continue to drop after DOMS inducing exercise[20][21], and the deficiency in glycogen lasts for over 72 hours[21].
- There are some studies that indicate there are possible changes in muscle fiber recruitment patterns[22][23][24].
7 How long does DOMS last?
It seems likely that exercise characteristics (duration, intensity, etc.) will change the time to recovery[25][26]. The soreness generally peaks between 24-72 hours after the damaging exercise, but will last at least 4 days[26]. My personal experience is that DOMS can last for over a week, and I prefer to avoid Downhill Running in the two weeks before a race, though sometimes I will include it as close as 10 days beforehand.
8 The effect of steepness on DOMS
I have found that steeper descents produce disproportionately severe DOMS. This might be due to the angle of the knee, as most[27][28] (but not all[26]) studies indicate that the longer a muscle is when being stressed, the greater the DOMS. This effect is most noticeable when using a Treadmill for Downhill Running, as small changes in angle can produce a big difference in DOMS.
9 How to prevent or treat DOMS?
There are various approaches to preventing or treating DOMS. The table below is a summary of the approaches showing how likely the strategy is to prevent or treat DOMS combined with the possible significant downsides. At the top are those that are likely to help and have no downsides, then those that have no effects or downsides, then those with little benefit and significant downsides.
| Strategy | Timing | Soreness | Weakness | Downsides |
|---|---|---|---|---|
| Repeated Bout Effect | Before (days to months) | Strong evidence of reduced soreness | Some evidence of reduced weakness | None |
| Carbohydrate and/or protein | After | Some evidence of reduced soreness | Strong evidence of reduced weakness | None |
| Cadence | During | Some evidence of reduced soreness | Some evidence of reduced soreness | None |
| Compression Clothing | After | Some evidence of reduced soreness | Some evidence of reduced weakness | None |
| Caffeine | After | Some evidence of reduced soreness | Some evidence of reduced weakness | Nonea |
| Massage | After | Some evidence of reduced soreness | Some evidence of reduced weakness | None |
| Warmup | Immediately before | Some evidence of reduced soreness | No benefit | None |
| Light Exercise | After | Transient pain reduction | No benefit | Nonec |
| TENS | After | Transient pain reduction | No benefit | None |
| Icing | After | No benefit | No benefit | Noneb |
| Antioxidents | Before and/or After | Mixed evidence | Mixed evidence | Conflicting evidence of reduced Endurance Adaptations |
| Stretching | Before and/or After | No benefit | No benefit | # Stretchingtemporarily weakens muscles
|
| NSAIDs | Before and/or After | Most evidence indicates no benefit | Most evidence indicates no benefit | Can impair recovery |
Notes
- aCaffeine can interfere with sleep
- b Only ever use ice in a bag, never a frozen gel pack. Gel packs start too cold and can cause skin or nerve damage.
- c Light exercise does not appear to speed up healing, but it does not hinder it either.
9.1 Repeated Bout Effect
The DOMS that follows an initial bout of eccentric exercise is much less on subsequent similar bouts. This is often called the Repeated Bout Effect (RBE)[15][13]. The initial bout does not have to cause significant soreness or damage[29]. As few as 2-10 maximal eccentric repetitions can protect against a subsequent larger bout (24-50), but the initial bout must be close to maximal effort[30]. By contrast, eight weeks of training with 50% of the maximal eccentric load did not provide protection against a subsequent maximal bout[31]. There is some cross-over of protection between different forms of exercise. For instance, eccentric weight training protects against soreness and weakness in subsequent downhill running[32]. The protection from the RBE is long lived. One study showed that while the initial weakness was not reduced by the RBE, the recovery of strength was much faster for up to 9 months, and soreness was less for up to 6 months[33]. Another study showed that 30 minutes of downhill running provides protection for between 6 and 9 weeks[34]. There is evidence that the RBE may rapidly start to provide protection from soreness and weakness[35], within 5 days[36], and possibly within 24 hours[37]. One study[38] demonstrated a change in the length-tension curve of DOMS trained muscles. As shown on the chart below, 7 days after a bout of DOMS inducing exercise the hamstring is able to generate more force and generate it at a greater angle.

9.1.1 Repeated Bout and Vitamin C
I found a single study that looked at how the repeated bout effect changes with Vitamin C[39]. As described below, most studies have found a small reduction in DOMS with Vitamin C. This 2014 study found that for the first bout, Vitamin C reduced the muscle soreness for the hamstrings, Quads, and Tibialis Anterior (shin), but the soreness of the glutes and calves were similar. However, for the second bout, not only was the soreness was reduced for the placebo, but it was further reduced with the Vitamin C. While this is just one study, it is intriguing with some profound implications. If the protective benefits of the repeated bout effect are dependent on nutritional (or other) factors, some runners may not get the benefit from their training. Personally, I've been taking ~1g/day of Vitamin C for many years due to skin condition. However, the evidence that Vitamin C impairs the adaptation to exercise caused me to take a break for about 15 months. During that break from Vitamin C, I found my ability to perform downhill running was quite impaired, and I didn't seem to be able to build up resistance from the repeated bout effect.

9.2 Carbohydrate and Protein
Main article: Nutrient Timing
The damage of DOMS requires repair, so it's not surprising that taking Protein or amino acids, which are the building blocks of the muscle fibers, helps with recovery.
- Most studies show that amino acids reduce muscle soreness[40][41] [42][43], and may[43][41] or may not reduce weakness[44][45][44].
- Most studies have shown that protein will reduce muscle weakness after DOMS inducing exercise[46][47] [48][49][50], with only two studies showing no improvement[51][52].
- The effect of protein on soreness is more mixed with some studies showing improvement[53] [54][50], but others not[46][55][52].
- Not surprisingly timing may be important, with CHO+PRO having an effect on muscle weakness directly after or 24 hours after, but not before DOMS inducing exercise[49], as shown below.
- In addition to reducing muscle soreness, protein supplementation in military recruits also reduced illness and injury[54].
- Taking carbohydrate alone after DOMS inducing exercise does not appear to help[56][57].

Protein helps with recovery from DOMS[50]. The graphs below show the impact of 100 grams of Protein taken immediately after 30 minutes of downhill running. Note that muscle soreness peaked at 72 hours, even though force and power had returned to baseline.


9.3 Cadence
Main article: Cadence
A study that looked at how changes in Cadence impacted the DOMS symptoms of downhill running showed that compared with a runner's preferred cadence, a higher cadence reduced subsequent weakness while a lower cadence increased soreness[58]. This change in DOMS is not surprising given that an increased cadence reduces the impact forces of running[59][60][61]. The impact forces from a lower cadence are mostly absorbed by the knee[62], which would create greater eccentric loading of the quads. In addition, most[27][28] (but not all[26]) studies show that the more extended a muscle is when undergoing eccentric stress, the more likely it is to suffer from DOMS. This is likely to compound the effect of Cadence on DOMS.
9.4 Compression Clothing
Main article: Why compression clothes
Studies show that wearing Graduated Compression Clothing during the days after DOMS inducing exercise mitigates the soreness[63][64][65][66][67][68][69] and weakness[64][66][67] of DOMS. Relatively few studies showed no benefit from compression clothing[70][71]. However, the results of compression clothing are likely to vary with the particular garment, how well it fits and therefore the pressure that is provided[72]. I found one studies that looked at the effect of wearing compression clothing during DOMS inducing exercise on the subsequent recovery[73]. This study used either or both graduated or uniform compression socks on hiking, a trail run, or calf exercise, with the socks also worn for the following four days. Graduated socks reduced DOMS pain on the hike compared with no compression, the only test with no compression as a control. The uniform compression reduced the pain compared with graduated on the run, and there was no difference between them on the calf exercise. This suggests to me that uniform compression might be better than graduated, or at least, it might not be worth paying extra for graduated compression.
9.5 Caffeine
Main article: Caffeine
Caffeine has shown to be effective in reducing the pain of DOMS, as well as reducing the weakness[74]. (The reduction in weakness did not reach statistical significance in regular caffeine users[75].) While the evidence for caffeine reducing the weakness of DOMS, this is one of the few approaches that can help offset the weakness during the damaging exercise.
9.6 Massage
Main article: Massage
Massage is widely used to prevent and treat injuries. Most meta-analysis suggest that post-exercise massage helps with the soreness of DOMS[76][77], though the mechanisms are unclear[78]. Studies that give massage 2-3 hours after DOMS inducing exercise showed reduced soreness[79][80][81], but not weakness[80][81]. One study that gave massage 2 days after exercise that resulted in reduced soreness and improved muscle function[82], but other studies that use massage 24 hours or more after exercise showed no benefit[83][84]. A study that used 20 minutes of foam rolling immediately following the DOMS inducing exercise, then again at 24 and 48 hours showed a significant improvement in both pain and muscular performance[14]. Therefore it seems likely that the timing of the massage is important, though other factors, such as the style of massage and the extent of the DOMS may also change the outcome. My personal experience suggests that massage immediately after the exercise is more effective than when the massage is delayed. (All too often, the muscles are too painful under pressure to allow any form of massage.)
9.7 Warmup
Main article: Warmup
Performing a Warmup before exercise may help reduce DOMS pain[85][86], but not all studies support this[87].
9.8 Light Exercise
Light training in the days following DOMS inducing exercise generally accepted to be one of the most effective ways of reducing muscle soreness, but unfortunately the reduction in pain is temporary[88][89][15][13]. A study that looked at running 30 minutes/day after DOMS inducing downhill running shows that the extra exercise neither helped nor hindered with soreness, weakness or Running Economy[90]. (The study only looked at the 7 days following the downhill running, and it would be interesting to know if there are any longer-term differences.) One study used cycling at light (30%) or moderate (70%) immediately after DOMS inducing exercise[91]. The moderate intensity cycling prevented the loss of strength, and actually increased strength on days 3 and 4. There were no differences between the control and the light exercise, nor between any of the conditions for soreness. This is an interesting suggestion that higher intensity exercise might be beneficial, but the study has a number of flaws, including the use of predicted Maximum Heart Rate to set exercise intensity.
9.9 TENS
TENS may reduce the soreness of DOMS[92], but the effect seems to be transient[93] and the effect is reduced if combined with icing[94]. Not all studies show any pain reduction[95] and none show a reduction in the weakness.
9.10 Icing
Main article: Cryotherapy
Sadly, Icing does not help with DOMS[96][97][98][11], and can make DOMS worse[99][100]. Ice reduces pain slightly, but does not restore strength[94]. (In my experience, ice can be extremely effective at helping heal muscle tears and non-DOMS muscle injuries, but not DOMS.)
9.11 Protracted Heat
One study looked at applying heat for 8 hours, either directly after DOMS inducing exercise or 24 hours later[101]. The study used "ThermaCare" chemically generated heat wraps, and I suspect the study was sponsored by the company. The 60 subjects underwent 5 minutes of squats to induce DOMS, then 20 were controls, 20 had immediate heat for 8 hours and the remainder had heat applied 24 hours after exercise. The immediate heat subjects had little reduction in strength over the follow three days, where the 24-hour delayed heat was no different from the controls. The strength drop was about 24% in controls/delayed-heat, which is a meaningful improvement. There was some reduction in pain over the first two days, with the immediate heat doing better than the delayed heat, which was slightly better than the controls.
9.12 Antioxidants - Vitamin C and E
The evidence for anti-oxidants is mixed, with some studies showing a benefit but not others. Note that one study below showed an impaired recovery with vitamin C supplementation. In addition, there is mixed evidence that vitamin C and/or vitamin E reduces Endurance Adaptations from exercise[102][103][104] or they do not[105][106] [107]. A 2019 systematic review of 50 studies covering 1,089 subjects concluded that there was moderate quality evidence that Vitamin C reduced DOMS at 48 and 96 hours, with lower quality evidence for 6 and 24 hours, but the reduction was quite small[108].
| Vitamin C | Vitamin E | Dose Period | Result |
|---|---|---|---|
| 3,000mg/day | 14 days prior and 4 days post-exercise | Vitamin C reduces soreness in first 24 hours[109] | |
| 3,000mg/day | 3 days prior and 4 days post-exercise | reduced soreness[110] | |
| 400mg/day | 14 days prior to exercise | reduced soreness[111] | |
| 3,000mg/day | 3 days prior and 5 days post-exercise | no effect[112] | |
| 1,000mg/day | 2 hours prior and 4 days post-exercise | no soreness change, but impaired strength recovery 7 and 14 days after exercise[113] | |
| 1,000mg | 2 hours prior to exercise | no effect[114] | |
| 400mg/day | 12 days prior and 3 days post-exercise | no change in soreness[115] | |
| 1,200 IU/day | 30 days prior to exercise | No effect[116] | |
| 500mg/day | 1,200 IU/day | 30 days prior and 7 days post-exercise | improved muscle function but no change in soreness[117] |
| 1,000mg/day | 300 mg/d | 6 weeks prior to exercise | no change in function[118] |
9.13 Stretching
Main article: Stretching
Stretching before[119][120] [121], after [120][122][123], or both before and after[124] exercise does not help with DOMS. In fact, stretching alone can induce DOMS[125]. Both static and dynamic stretching are ineffective[126].
9.14 NSAIDs
Main article: NSAIDs and Running
The most common NSAIDs (Ibuprofen, Acetaminophen/Paracetamol, and Aspirin) are unlikely to help with DOMS, but Naproxen may reduce the pain and weakness. If an NSAID is taken, it should probably be immediately after the damaging exercise rather than waiting until the soreness develops. It seems likely that taking an NSAID for DOMS will reduce the muscular growth that would normally occur as part of the recovery. In one disturbing study, rabbits treated with an NSAID (flurbiprofen) after DOMS inducing exercise initially recovered their strength after 3-7 days, but between days 7 and 28 days the rabbits became weaker while the untreated controls became stronger[127]. I have not included other animal studies, but this is the only one that looks at how NSAIDs impact the longer term recovery from DOMS. Studies of Turmeric, which acts as a selective COX-2 NSAID[128], are promising. Reduction in soreness is mixed, with some studies showing reduced soreness[129][130] [131], while others do not[132][133]. However, one study shoes reduced weakness and inflammation markers[133] and an animal study showed less subsequent reduction in running performance in mice[134]. Several studies showed reduced markers of damage[135][134][133][132] [131]. However, Turmeric should be treated like any other medication as there are safety concerns; see Turmeric as an NSAID for details.
| NSAID | Soreness | Weakness |
|---|---|---|
| Ibuprofen | 2xImproved[136][137] | 1xMaybe[136] |
| Ibuprofen Gel | 1xNo Effect[144] | |
| Acetaminophen (Paracetamol) | 2xNo Effect[145][146] | |
| Aspirin | 2xImproved[147][148] | 2xNo Effect[147][148] |
| Naproxen | 4xImproved[149][150][151][152]
1xNo Effect[153] |
3xImproved[149][150][151]
1xNo Effect[153] |
| Diclofenac | Possible slight reduction[154] | |
| Codeine | 1xNo Effect[145] | |
| Rofecoxib | 1xNo Effect[155] | |
| Ketoprofen | 1xImproved[156] | 1xImproved[156] |
| Bromelain | 1xNo Effect[143] | |
| Turmeric | 2xImproved[129][130] | 2xImproved[133][134] |
9.15 CBD Oil
I have heard anecdotal suggestions that CBD oil may help with sleep after DOMS inducing exercise, but I've found no supporting research. Note that in 2018, World Anti-Doping Agency (WADA) removed CBD, from its 2018 prohibited substances list, but the legality of CBD is complex.
10 Menstrual Cycle
A study has shown that DOMS does not vary with menstrual cycle[157].
11 Mechanisms of DOMS
The underlying mechanism of DOMS is thought to consist of phases; the initial damage that occurs during the exercise and then secondary damage that occurs subsequently[13][15]:
- Primary damage. The initial damage is believed to be mechanical in nature, both on the contracting parts of the muscle (sarcomeres) and the supporting structures (primarily the z-bands). While there are some suggestions that the primary damage might be due to metabolic factors such as low blood flow, low oxygen saturation, impaired metabolite clearance, these causes are not well supported. The idea that DOMS is caused by lactic acid has been rejected[158].
- Secondary damage. The secondary damage appears to be initiated by the disruption of the intracellular Ca2+homeostatis, which leads to further myofibrillar damage including degradation of the cell membrane.
11.1 Mechanisms for the Repeated Bout Effect
For those interested in the details, there are several possible mechanisms that might be responsible for the Repeated Bout Effect (RBE)[159][160]:
- Neural adaptation. The RBE may be due to changes in the way muscles are recruited. While there is some direct evidence that RBE occurs without neural adaptations, it is possible that this mechanism contributes to the protection.
- Increased recruitment of slow-twitch fibers. Fast-twitch fibers may be more susceptible to eccentric damage, so an adaptation to recruit more slow-twitch fibers might reduce DOMS.
- Activation of more muscle fibers. Recruiting a larger number of fibers may reduce the eccentric stress on each fiber, thus reducing the damage.
- Mechanical adaptation. It is possible to consider muscle damage as similar to materials fatigue. These adaptations are in the non-contracting structures of the muscles. For instance, protection from damage could come from increased structural strength in the z-band of the muscles which get disturbed by eccentric exercise as seen above.
- Increased dynamic muscle stiffness. Dynamic stiffness refers to how stiff the muscles are when contracted.
- Increased passive muscle stiffness. In contrast, passive stiffness is when the muscles are relaxed. It is unclear if increased passive stiffness protects against eccentric damage or actually exacerbates it.
- Cellular adaptation. A number of changes at the cellular level may provide protection against eccentric damage.
- Increased sarcomeres. The sarcomeres are part of the contracting mechanism of the muscles. The contraction of a muscle comes from parts of the sarcomere sliding over each other. One adaptation to eccentric exercise may be that the overlap in these sliding areas becomes larger. A study in rats suggests that the adaptation may include more sarcomeres in series, which produces a greater Range Of Motion and greater force at longer muscle lengths[161].
- Changed inflammation response. The delay in soreness is probably due to a delayed inflammatory response, so changes in that response could reduce the soreness. However, this would not reduce the immediate loss of strength.
- Maintenance of Excitation-Contraction coupling. One reason for the loss of strength following eccentric exercise is that the nerve impulses (excitation) may result in less contraction. The decoupling could be due to lack of neural drive (perhaps due to pain), physical disruption of the contracting structures of the muscle, or a failure to activate those contracting structures.
12 Limitations of the current scientific studies
While there are a large number of scientific studies available on DOMS, these studies have a number of limitations.
- Most studies use a small number of subjects, limiting their ability to detect the effectiveness of treatments.
- The studies are not consistent in the level of DOMS that is provoked, with some studies having relatively mild soreness.
- Not all studies avoid the confounding effects of the Repeated Bout Effect. This can be where the study has not ensured that subjects have not performed any eccentric exercise in the recent past, or where subjects undergo multiple bouts in the study.
- The studies generally do not establish any dose/response relationship.
- Human studies are limited in their timeframe, so that the longer term effects of the treatments are unclear.
- Studies often focus on how a treatment reduces the symptoms of DOMS without looking at how the treatment might also change the adaptation process. A DOMS treatment that effectively reduces soreness and/or weakness but also prevents any adaptation to the training has limited benefit.
13 See Also
14 References
- ↑ 1.0 1.1 Andrew J Vickers, BMC Musculoskeletal Disorders, volume 2, issue 1, 2001, pages 5, ISSN 14712474, doi 10.1186/1471-2474-2-5
- ↑ L Feasson, D Stockholm, D Freyssenet, I Richard, S Duguez, J S Beckmann, C Denis, Molecular adaptations of neuromuscular disease-associated proteins in response to eccentric exercise in human skeletal muscle, The Journal of Physiology, volume 543, issue 1, 2002, pages 297–306, ISSN 0022-3751, doi 10.1113/jphysiol.2002.018689
- ↑ MJ. Warhol, AJ. Siegel, WJ. Evans, LM. Silverman, Skeletal muscle injury and repair in marathon runners after competition., Am J Pathol, volume 118, issue 2, pages 331-9, Feb 1985, PMID 3970143
- ↑ V. Marginson, AV. Rowlands, NP. Gleeson, RG. Eston, Comparison of the symptoms of exercise-induced muscle damage after an initial and repeated bout of plyometric exercise in men and boys., J Appl Physiol, volume 99, issue 3, pages 1174-81, Sep 2005, doi 10.1152/japplphysiol.01193.2004, PMID 15817716
- ↑ Skeletal muscle damage and repair http://books.google.com/books?id=ueMh1x7kFjsC&lpg=PA195&ots=wwIhuoi0Nt&dq=Tiidus%201997&pg=PA69#v=onepage&q=Tiidus%201997&f=true
- ↑ FM. Impellizzeri, NA. Maffiuletti, Convergent evidence for construct validity of a 7-point likert scale of lower limb muscle soreness., Clin J Sport Med, volume 17, issue 6, pages 494-6, Nov 2007, doi 10.1097/JSM.0b013e31815aed57, PMID 17993794
- ↑ Kazunori Nosaka, Mike Newton, Paul Sacco, Delayed-onset muscle soreness does not reflect the magnitude of eccentric exercise-induced muscle damage, Scandinavian Journal of Medicine & Science in Sports, volume 12, issue 6, 2002, pages 337–346, ISSN 09057188, doi 10.1034/j.1600-0838.2002.10178.x
- ↑ 8.0 8.1 8.2 JM. Saxton, PM. Clarkson, R. James, M. Miles, M. Westerfer, S. Clark, AE. Donnelly, Neuromuscular dysfunction following eccentric exercise., Med Sci Sports Exerc, volume 27, issue 8, pages 1185-93, Aug 1995, PMID 7476064
- ↑ 9.0 9.1 Delayed Onset Muscle Soreness and Decreased Isokinetic Stren... : The Journal of Strength & Conditioning Research http://journals.lww.com/nsca-jscr/abstract/1988/05000/delayed_onset_muscle_soreness_and_decreased.1.aspx
- ↑ 10.0 10.1 DT. Gulick, IF. Kimura, M. Sitler, A. Paolone, JD. Kelly, Various treatment techniques on signs and symptoms of delayed onset muscle soreness., J Athl Train, volume 31, issue 2, pages 145-52, Apr 1996, PMID 16558388
- ↑ 11.0 11.1 DJ. Paddon-Jones, BM. Quigley, Effect of cryotherapy on muscle soreness and strength following eccentric exercise., Int J Sports Med, volume 18, issue 8, pages 588-93, Nov 1997, doi 10.1055/s-2007-972686, PMID 9443590
- ↑ 12.0 12.1 A. Baldwin Lanier, Use of nonsteroidal anti-inflammatory drugs following exercise-induced muscle injury., Sports Med, volume 33, issue 3, pages 177-85, 2003, PMID 12656639
- ↑ 13.0 13.1 13.2 13.3 K. Cheung, P. Hume, L. Maxwell, Delayed onset muscle soreness : treatment strategies and performance factors., Sports Med, volume 33, issue 2, pages 145-64, 2003, PMID 12617692
- ↑ 14.0 14.1 GE. Pearcey, DJ. Bradbury-Squires, JE. Kawamoto, EJ. Drinkwater, DG. Behm, DC. Button, Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures., J Athl Train, volume 50, issue 1, pages 5-13, Jan 2015, doi 10.4085/1062-6050-50.1.01, PMID 25415413
- ↑ 15.0 15.1 15.2 15.3 15.4 G. Howatson, KA. van Someren, The prevention and treatment of exercise-induced muscle damage., Sports Med, volume 38, issue 6, pages 483-503, 2008, PMID 18489195
- ↑ Muscle Soreness During Running: Biomechanical and Physiological Considerations http://journals.humankinetics.com/jab-back-issues/jabvolume7issue2may/musclesorenessduringrunningbiomechanicalandphysiologicalconsiderations
- ↑ 17.0 17.1 Smith LL. Causes of delayed onset muscle soreness and the impact on athletic performance: a review. J Appl Sport Sci Res 1992; 6 (3): 135-41
- ↑ 18.0 18.1 WA. Braun, DJ. Dutto, The effects of a single bout of downhill running and ensuing delayed onset of muscle soreness on running economy performed 48 h later., Eur J Appl Physiol, volume 90, issue 1-2, pages 29-34, Sep 2003, doi 10.1007/s00421-003-0857-8, PMID 12783232
- ↑ DL. Costill, DD. Pascoe, WJ. Fink, RA. Robergs, SI. Barr, D. Pearson, Impaired muscle glycogen resynthesis after eccentric exercise., J Appl Physiol, volume 69, issue 1, pages 46-50, Jul 1990, PMID 2394662
- ↑ M. Zehnder, M. Muelli, R. Buchli, G. Kuehne, U. Boutellier, Further glycogen decrease during early recovery after eccentric exercise despite a high carbohydrate intake., Eur J Nutr, volume 43, issue 3, pages 148-59, Jun 2004, doi 10.1007/s00394-004-0453-7, PMID 15168037
- ↑ 21.0 21.1 JJ. Widrick, DL. Costill, GK. McConell, DE. Anderson, DR. Pearson, JJ. Zachwieja, Time course of glycogen accumulation after eccentric exercise., J Appl Physiol, volume 72, issue 5, pages 1999-2004, May 1992, PMID 1601811
- ↑ MP. Miles, JC. Ives, KR. Vincent, Neuromuscular control following maximal eccentric exercise., Eur J Appl Physiol Occup Physiol, volume 76, issue 4, pages 368-74, 1997, PMID 9349654
- ↑ S. Zhou, MF. Carey, RJ. Snow, DL. Lawson, WE. Morrison, Effects of muscle fatigue and temperature on electromechanical delay., Electromyogr Clin Neurophysiol, volume 38, issue 2, pages 67-73, Mar 1998, PMID 9553743
- ↑ S. Zhou, Acute effect of repeated maximal isometric contraction on electromechanical delay of knee extensor muscle., J Electromyogr Kinesiol, volume 6, issue 2, pages 117-27, Jun 1996, PMID 20719669
- ↑ AJ. Vickers, Time course of muscle soreness following different types of exercise., BMC Musculoskelet Disord, volume 2, pages 5, 2001, PMID 11701094
- ↑ 26.0 26.1 26.2 26.3 V. Paschalis, Y. Koutedakis, AZ. Jamurtas, V. Mougios, V. Baltzopoulos, Equal volumes of high and low intensity of eccentric exercise in relation to muscle damage and performance., J Strength Cond Res, volume 19, issue 1, pages 184-8, Feb 2005, doi 10.1519/R-14763.1, PMID 15705032 Cite error: Invalid
<ref>tag; name "Paschalis-2005" defined multiple times with different content - ↑ 27.0 27.1 DA. Jones, DJ. Newham, C. Torgan, Mechanical influences on long-lasting human muscle fatigue and delayed-onset pain., J Physiol, volume 412, pages 415-27, May 1989, PMID 2600839
- ↑ 28.0 28.1 RB. Child, JM. Saxton, AE. Donnelly, Comparison of eccentric knee extensor muscle actions at two muscle lengths on indices of damage and angle-specific force production in humans., J Sports Sci, volume 16, issue 4, pages 301-8, May 1998, doi 10.1080/02640419808559358, PMID 9663954
- ↑ PM. Clarkson, WC. Byrnes, E. Gillisson, E. Harper, Adaptation to exercise-induced muscle damage., Clin Sci (Lond), volume 73, issue 4, pages 383-6, Oct 1987, PMID 3665359
- ↑ SJ. Brown, RB. Child, SH. Day, AE. Donnelly, Exercise-induced skeletal muscle damage and adaptation following repeated bouts of eccentric muscle contractions., J Sports Sci, volume 15, issue 2, pages 215-22, Apr 1997, doi 10.1080/026404197367498, PMID 9258852
- ↑ K. Nosaka, M. Newton, Concentric or eccentric training effect on eccentric exercise-induced muscle damage., Med Sci Sports Exerc, volume 34, issue 1, pages 63-9, Jan 2002, PMID 11782649
- ↑ RG. Eston, S. Finney, S. Baker, V. Baltzopoulos, Muscle tenderness and peak torque changes after downhill running following a prior bout of isokinetic eccentric exercise., J Sports Sci, volume 14, issue 4, pages 291-9, Aug 1996, doi 10.1080/02640419608727714, PMID 8887208
- ↑ K. Nosaka, K. Sakamoto, M. Newton, P. Sacco, How long does the protective effect on eccentric exercise-induced muscle damage last?, Med Sci Sports Exerc, volume 33, issue 9, pages 1490-5, Sep 2001, PMID 11528337
- ↑ WC. Byrnes, PM. Clarkson, JS. White, SS. Hsieh, PN. Frykman, RJ. Maughan, Delayed onset muscle soreness following repeated bouts of downhill running., J Appl Physiol, volume 59, issue 3, pages 710-5, Sep 1985, PMID 4055561
- ↑ J. Mair, M. Mayr, E. Müller, A. Koller, C. Haid, E. Artner-Dworzak, C. Calzolari, C. Larue, B. Puschendorf, Rapid adaptation to eccentric exercise-induced muscle damage., Int J Sports Med, volume 16, issue 6, pages 352-6, Aug 1995, doi 10.1055/s-2007-973019, PMID 7591384
- ↑ CB. Ebbeling, PM. Clarkson, Exercise-induced muscle damage and adaptation., Sports Med, volume 7, issue 4, pages 207-34, Apr 1989, PMID 2657962
- ↑ TC. Chen, SS. Hsieh, Effects of a 7-day eccentric training period on muscle damage and inflammation., Med Sci Sports Exerc, volume 33, issue 10, pages 1732-8, Oct 2001, PMID 11581559
- ↑ CL. Brockett, DL. Morgan, U. Proske, Human hamstring muscles adapt to eccentric exercise by changing optimum length., Med Sci Sports Exerc, volume 33, issue 5, pages 783-90, May 2001, PMID 11323549
- ↑ F. He, J. Hockemeyer, D. Sedlock, Does Combined Antioxidant Vitamin Supplementation Blunt Repeated Bout Effect?, International Journal of Sports Medicine, volume 36, issue 05, 2015, pages 407–413, ISSN 0172-4622, doi 10.1055/s-0034-1395630
- ↑ Glyn Howatson, Michael Hoad, Stuart Goodall, Jamie Tallent, Phillip G Bell, Duncan N French, Exercise-induced muscle damage is reduced in resistance-trained males by branched chain amino acids: a randomized, double-blind, placebo controlled study, Journal of the International Society of Sports Nutrition, volume 9, issue 1, 2012, pages 20, ISSN 1550-2783, doi 10.1186/1550-2783-9-20
- ↑ 41.0 41.1 BK. Greer, JL. Woodard, JP. White, EM. Arguello, EM. Haymes, Branched-chain amino acid supplementation and indicators of muscle damage after endurance exercise., Int J Sport Nutr Exerc Metab, volume 17, issue 6, pages 595-607, Dec 2007, PMID 18156664
- ↑ K. Matsumoto, T. Koba, K. Hamada, M. Sakurai, T. Higuchi, H. Miyata, Branched-chain amino acid supplementation attenuates muscle soreness, muscle damage and inflammation during an intensive training program., J Sports Med Phys Fitness, volume 49, issue 4, pages 424-31, Dec 2009, PMID 20087302
- ↑ 43.0 43.1 Y. Shimomura, A. Inaguma, S. Watanabe, Y. Yamamoto, Y. Muramatsu, G. Bajotto, J. Sato, N. Shimomura, H. Kobayashi, Branched-chain amino acid supplementation before squat exercise and delayed-onset muscle soreness., Int J Sport Nutr Exerc Metab, volume 20, issue 3, pages 236-44, Jun 2010, PMID 20601741
- ↑ 44.0 44.1 SR. Jackman, OC. Witard, AE. Jeukendrup, KD. Tipton, Branched-chain amino acid ingestion can ameliorate soreness from eccentric exercise., Med Sci Sports Exerc, volume 42, issue 5, pages 962-70, May 2010, doi 10.1249/MSS.0b013e3181c1b798, PMID 19997002
- ↑ K. Nosaka, P. Sacco, K. Mawatari, Effects of amino acid supplementation on muscle soreness and damage., Int J Sport Nutr Exerc Metab, volume 16, issue 6, pages 620-35, Dec 2006, PMID 17342883
- ↑ 46.0 46.1 Emma Cockburn, Philip R. Hayes, Duncan N. French, Emma Stevenson, Alan St Clair Gibson, Acute milk-based protein–CHO supplementation attenuates exercise-induced muscle damage, Applied Physiology, Nutrition, and Metabolism, volume 33, issue 4, 2008, pages 775–783, ISSN 1715-5312, doi 10.1139/H08-057
- ↑ RJ. Valentine, MJ. Saunders, MK. Todd, TG. St Laurent, Influence of carbohydrate-protein beverage on cycling endurance and indices of muscle disruption., Int J Sport Nutr Exerc Metab, volume 18, issue 4, pages 363-78, Aug 2008, PMID 18708686
- ↑ Matthew B Cooke, Emma Rybalka, Christos G Stathis, Paul J Cribb, Alan Hayes, Whey protein isolate attenuates strength decline after eccentrically-induced muscle damage in healthy individuals, Journal of the International Society of Sports Nutrition, volume 7, issue 1, 2010, pages 30, ISSN 1550-2783, doi 10.1186/1550-2783-7-30
- ↑ 49.0 49.1 49.2 E. Cockburn, E. Stevenson, PR. Hayes, P. Robson-Ansley, G. Howatson, Effect of milk-based carbohydrate-protein supplement timing on the attenuation of exercise-induced muscle damage., Appl Physiol Nutr Metab, volume 35, issue 3, pages 270-7, Jun 2010, doi 10.1139/H10-017, PMID 20555370
- ↑ 50.0 50.1 50.2 T. Etheridge, A. Philp, PW. Watt, A single protein meal increases recovery of muscle function following an acute eccentric exercise bout., Appl Physiol Nutr Metab, volume 33, issue 3, pages 483-8, Jun 2008, doi 10.1139/H08-028, PMID 18461101
- ↑ JR. Wojcik, J. Walber-Rankin, LL. Smith, FC. Gwazdauskas, Comparison of carbohydrate and milk-based beverages on muscle damage and glycogen following exercise., Int J Sport Nutr Exerc Metab, volume 11, issue 4, pages 406-19, Dec 2001, PMID 11915776
- ↑ 52.0 52.1 MS. Green, BT. Corona, JA. Doyle, CP. Ingalls, Carbohydrate-protein drinks do not enhance recovery from exercise-induced muscle injury., Int J Sport Nutr Exerc Metab, volume 18, issue 1, pages 1-18, Feb 2008, PMID 18272930
- ↑ ND. Luden, MJ. Saunders, MK. Todd, Postexercise carbohydrate-protein- antioxidant ingestion decreases plasma creatine kinase and muscle soreness., Int J Sport Nutr Exerc Metab, volume 17, issue 1, pages 109-23, Feb 2007, PMID 17460336
- ↑ 54.0 54.1 PJ. Flakoll, T. Judy, K. Flinn, C. Carr, S. Flinn, Postexercise protein supplementation improves health and muscle soreness during basic military training in Marine recruits., J Appl Physiol, volume 96, issue 3, pages 951-6, Mar 2004, doi 10.1152/japplphysiol.00811.2003, PMID 14657039
- ↑ A. Samadi, AA. Gaeini, MR. Kordi, M. Rahimi, N. Rahnama, E. Bambaeichi, Effect of various ratios of carbohydrate-protein supplementation on resistance exercise-induced muscle damage., J Sports Med Phys Fitness, volume 52, issue 2, pages 151-7, Apr 2012, PMID 22525650
- ↑ G L Close, Effects of dietary carbohydrate on delayed onset muscle soreness and reactive oxygen species after contraction induced muscle damage, British Journal of Sports Medicine, volume 39, issue 12, 2005, pages 948–953, ISSN 0306-3674, doi 10.1136/bjsm.2005.019844
- ↑ MR. Nelson, RK. Conlee, AC. Parcell, Inadequate carbohydrate intake following prolonged exercise does not increase muscle soreness after 15 minutes of downhill running., Int J Sport Nutr Exerc Metab, volume 14, issue 2, pages 171-84, Apr 2004, PMID 15118191
- ↑ Ann V. Rowlands, Roger G. Eston, Caroline Tilzey, Effect of stride length manipulation on symptoms of exercise-induced muscle damage and the repeated bout effect, Journal of Sports Sciences, volume 19, issue 5, 2001, pages 333–340, ISSN 0264-0414, doi 10.1080/02640410152006108
- ↑ JA. Mercer, P. Devita, TR. Derrick, BT. Bates, Individual effects of stride length and frequency on shock attenuation during running., Med Sci Sports Exerc, volume 35, issue 2, pages 307-13, Feb 2003, doi 10.1249/01.MSS.0000048837.81430.E7, PMID 12569221
- ↑ Hamill, J., T. R. Derrick, and K. G. Holt. "Shock attenuation and stride frequency during running." Human Movement Science 14.1 (1995): 45-60.
- ↑ TE. Clarke, LB. Cooper, CL. Hamill, DE. Clark, The effect of varied stride rate upon shank deceleration in running., J Sports Sci, volume 3, issue 1, pages 41-9, 1985, doi 10.1080/02640418508729731, PMID 4094019
- ↑ TR. Derrick, J. Hamill, GE. Caldwell, Energy absorption of impacts during running at various stride lengths., Med Sci Sports Exerc, volume 30, issue 1, pages 128-35, Jan 1998, PMID 9475654
- ↑ Vanessa Davies, Kevin G Thompson, Stephen-Mark Cooper, The Effects of Compression Garments on Recovery, Journal of Strength and Conditioning Research, volume 23, issue 6, 2009, pages 1786–1794, ISSN 1064-8011, doi 10.1519/JSC.0b013e3181b42589
- ↑ 64.0 64.1 WJ. Kraemer, JA. Bush, RB. Wickham, CR. Denegar, AL. Gómez, LA. Gotshalk, ND. Duncan, JS. Volek, M. Putukian, Influence of compression therapy on symptoms following soft tissue injury from maximal eccentric exercise., J Orthop Sports Phys Ther, volume 31, issue 6, pages 282-90, Jun 2001, PMID 11411623
- ↑ WJ. Kraemer, JA. Bush, RB. Wickham, Continuous Compression as an Effective Therapeutic Intervention in Treating Eccentric-Exercise-Induced Muscle Soreness, J Sport Rehab, volume 10, issue 1, pages 11-23, 2001
- ↑ 66.0 66.1 William J Kraemer, Shawn D Flanagan, Brett A Comstock, Maren S Fragala, Jacob E Earp, Courtenay Dunn-Lewis, Jen-Yu Ho, Gwendolyn A Thomas, Glenn Solomon-Hill, Zachary R Penwell, Matthew D Powell, Megan R Wolf, Jeff S Volek, Craig R Denegar, Carl M Maresh, Effects of a Whole Body Compression Garment on Markers of Recovery After a Heavy Resistance Workout in Men and Women, Journal of Strength and Conditioning Research, volume 24, issue 3, 2010, pages 804–814, ISSN 1064-8011, doi 10.1519/JSC.0b013e3181d33025
- ↑ 67.0 67.1 JR. Jakeman, C. Byrne, RG. Eston, Lower limb compression garment improves recovery from exercise-induced muscle damage in young, active females., Eur J Appl Physiol, volume 109, issue 6, pages 1137-44, Aug 2010, doi 10.1007/s00421-010-1464-0, PMID 20376479
- ↑ V. Davies, KG. Thompson, SM. Cooper, The effects of compression garments on recovery., J Strength Cond Res, volume 23, issue 6, pages 1786-94, Sep 2009, doi 10.1519/JSC.0b013e3181b42589, PMID 19675482
- ↑ R. Duffield, M. Portus, J. Edge, Comparison of three types of full-body compression garments on throwing and repeat-sprint performance in cricket players * COMMENTARY, British Journal of Sports Medicine, volume 41, issue 7, 2007, pages 409–414, ISSN 0306-3674, doi 10.1136/bjsm.2006.033753
- ↑ Jon Carling, Kennon Francis, Christopher Lorish, The effects of continuous external compression on delayed-onset muscle soreness (DOMS), International Journal of Rehabilitation and Health, volume 1, issue 4, 1995, pages 223–235, ISSN 1068-9591, doi 10.1007/BF02214641
- ↑ Pearce, Alan J., et al. "Wearing a sports compression garment on the performance of visuomotor tracking following eccentric exercise: A pilot study." Journal of science and medicine in sport 12.4 (2009): 500-502.
- ↑ BA. MacRae, JD. Cotter, RM. Laing, Compression garments and exercise: garment considerations, physiology and performance., Sports Med, volume 41, issue 10, pages 815-43, Oct 2011, doi 10.2165/11591420-000000000-00000, PMID 21923201
- ↑ Adam C McDonnell, Diane Cooper, Tinkara Mlinar, Igor B Mekjavic, The effect of post-exercise application of either graduated or uniform compression socks on the mitigation of delayed onset muscle soreness, Textile Research Journal, 2018, pages 004051751878000, ISSN 0040-5175, doi 10.1177/0040517518780002
- ↑ V. Maridakis, PJ. O'Connor, GA. Dudley, KK. McCully, Caffeine attenuates delayed-onset muscle pain and force loss following eccentric exercise., J Pain, volume 8, issue 3, pages 237-43, Mar 2007, doi 10.1016/j.jpain.2006.08.006, PMID 17161977
- ↑ ND. Park, RD. Maresca, KI. McKibans, DR. Morgan, TS. Allen, GL. Warren, Caffeines enhancement of maximal voluntary strength and activation in uninjured but not injured muscle., Int J Sport Nutr Exerc Metab, volume 18, issue 6, pages 639-52, Dec 2008, PMID 19164833
- ↑ E. Ernst, Does post-exercise massage treatment reduce delayed onset muscle soreness? A systematic review., Br J Sports Med, volume 32, issue 3, pages 212-4, Sep 1998, PMID 9773168
- ↑ A. Moraska, Sports massage. A comprehensive review., J Sports Med Phys Fitness, volume 45, issue 3, pages 370-80, Sep 2005, PMID 16230990
- ↑ PM. Tiidus, Manual massage and recovery of muscle function following exercise: a literature review., J Orthop Sports Phys Ther, volume 25, issue 2, pages 107-12, Feb 1997, PMID 9007768
- ↑ LL. Smith, MN. Keating, D. Holbert, DJ. Spratt, MR. McCammon, SS. Smith, RG. Israel, The effects of athletic massage on delayed onset muscle soreness, creatine kinase, and neutrophil count: a preliminary report., J Orthop Sports Phys Ther, volume 19, issue 2, pages 93-9, Feb 1994, PMID 8148868
- ↑ 80.0 80.1 Z. Zainuddin, M. Newton, P. Sacco, K. Nosaka, Effects of massage on delayed-onset muscle soreness, swelling, and recovery of muscle function., J Athl Train, volume 40, issue 3, pages 174-80, PMID 16284637
- ↑ 81.0 81.1 J E Hilbert, The effects of massage on delayed onset muscle soreness, British Journal of Sports Medicine, volume 37, issue 1, 2003, pages 72–75, ISSN 03063674, doi 10.1136/bjsm.37.1.72
- ↑ Corrie A. Mancinelli, D. Scott Davis, Leila Aboulhosn, Misty Brady, Justin Eisenhofer, Stephanie Foutty, The effects of massage on delayed onset muscle soreness and physical performance in female collegiate athletes, Physical Therapy in Sport, volume 7, issue 1, 2006, pages 5–13, ISSN 1466853X, doi 10.1016/j.ptsp.2005.10.004
- ↑ JM. Hart, CB. Swanik, RT. Tierney, Effects of sport massage on limb girth and discomfort associated with eccentric exercise., J Athl Train, volume 40, issue 3, pages 181-5, PMID 16284638
- ↑ LG. Dawson, PM. Dawson, PM. Tiidus, Evaluating the influence of massage on leg strength, swelling, and pain following a half-marathon., J Sports Sci Med, pages 37-43, 2004
- ↑ RY. Law, RD. Herbert, Warm-up reduces delayed onset muscle soreness but cool-down does not: a randomised controlled trial., Aust J Physiother, volume 53, issue 2, pages 91-5, 2007, PMID 17535144
- ↑ 86.0 86.1 86.2 N Rahnama, F Rahmani-Nia, K Ebrahim, The isolated and combined effects of selected physical activity and ibuprofen on delayed-onset muscle soreness, Journal of Sports Sciences, volume 23, issue 8, 2005, pages 843–850, ISSN 0264-0414, doi 10.1080/02640410400021989
- ↑ RK. Evans, KL. Knight, DO. Draper, AC. Parcell, Effects of warm-up before eccentric exercise on indirect markers of muscle damage., Med Sci Sports Exerc, volume 34, issue 12, pages 1892-9, Dec 2002, doi 10.1249/01.MSS.0000038895.14935.C8, PMID 12471293
- ↑ RB. Armstrong, Mechanisms of exercise-induced delayed onset muscular soreness: a brief review., Med Sci Sports Exerc, volume 16, issue 6, pages 529-38, Dec 1984, PMID 6392811
- ↑ Z. Zainuddin, P. Sacco, M. Newton, K. Nosaka, Light concentric exercise has a temporarily analgesic effect on delayed-onset muscle soreness, but no effect on recovery from eccentric exercise., Appl Physiol Nutr Metab, volume 31, issue 2, pages 126-34, Apr 2006, doi 10.1139/h05-010, PMID 16604130
- ↑ Trevor C. Chen, Kazunori Nosaka, Chia-Ching Wu, Effects of a 30-min running performed daily after downhill running on recovery of muscle function and running economy, Journal of Science and Medicine in Sport, volume 11, issue 3, 2008, pages 271–279, ISSN 14402440, doi 10.1016/j.jsams.2007.02.015
- ↑ James J. Tufano, Lee E. Brown, Jared W. Coburn, Kavin K.W. Tsang, Vanessa L. Cazas, Joe W. LaPorta, Effect of Aerobic Recovery Intensity on Delayed-Onset Muscle Soreness and Strength, Journal of Strength and Conditioning Research, volume 26, issue 10, 2012, pages 2777–2782, ISSN 1064-8011, doi 10.1519/JSC.0b013e3182651c06
- ↑ CR. Denegar, DH. Perrin, AD. Rogol, RA. Rutt, Influence of transcutaneous electrical nerve stimulation on pain, range of motion, and serum cortisol concentration in females experiencing delayed onset muscle soreness., J Orthop Sports Phys Ther, volume 11, issue 3, pages 100-3, 1989, PMID 18796921
- ↑ The Effects of Low-Volt, Microamperage Stimulation on Delayed Onset Muscle Soreness http://journals.humankinetics.com/jsr-back-issues/jsrvolume1issue2may/theeffectsoflowvoltmicroamperagestimulationondelayedonsetmusclesoreness
- ↑ 94.0 94.1 CR. Denegar, DH. Perrin, Effect of transcutaneous electrical nerve stimulation, cold, and a combination treatment on pain, decreased range of motion, and strength loss associated with delayed onset muscle soreness., J Athl Train, volume 27, issue 3, pages 200-6, 1992, PMID 16558162
- ↑ JA. Bonacci, EJ. Higbie, Effects of microcurrent treatment on perceived pain and muscle strength following eccentric exercise., J Athl Train, volume 32, issue 2, pages 119-23, Apr 1997, PMID 16558440
- ↑ L. Yackzan, C. Adams, KT. Francis, The effects of ice massage on delayed muscle soreness., Am J Sports Med, volume 12, issue 2, pages 159-65, PMID 6742292
- ↑ CiNii Articles - EFFECTS OF ICE PACK ON MUSCLE INJURY INDUCED BY ECCENTRIC CONTRACTIONS http://ci.nii.ac.jp/naid/110004787806
- ↑ Delayed Onset Muscle Soreness: What Is It and How Do We Treat It? http://journals.humankinetics.com/jsr-back-issues/jsrvolume5issue3august/delayedonsetmusclesorenesswhatisitandhowdowetreatit
- ↑ Ching-Yu Tseng, Jo-Ping Lee, Yung-Shen Tsai, Shin-Da Lee, Chung-Lan Kao, Te-Chih Liu, Cheng-Shou Lai, M. Brennan Harris, Chia-Hua Kuo, Topical Cooling (Icing) Delays Recovery from Eccentric Exercise-Induced Muscle Damage, Journal of Strength and Conditioning Research, 2012, pages 1, ISSN 1064-8011, doi 10.1519/JSC.0b013e318267a22c
- ↑ WK. Isabell, E. Durrant, W. Myrer, S. Anderson, The effects of ice massage, ice massage with exercise, and exercise on the prevention and treatment of delayed onset muscle soreness., J Athl Train, volume 27, issue 3, pages 208-17, 1992, PMID 16558163
- ↑ Jerrold Petrofsky, Lee Berk, Gurinder Bains, Iman Akef Khowailed, Haneul Lee, Michael Laymon, The Efficacy of Sustained Heat Treatment on Delayed-Onset Muscle Soreness, Clinical Journal of Sport Medicine, volume 27, issue 4, 2017, pages 329–337, ISSN 1050-642X, doi 10.1097/JSM.0000000000000375
- ↑ MC. Gomez-Cabrera, E. Domenech, M. Romagnoli, A. Arduini, C. Borras, FV. Pallardo, J. Sastre, J. Viña, Oral administration of vitamin C decreases muscle mitochondrial biogenesis and hampers training-induced adaptations in endurance performance., Am J Clin Nutr, volume 87, issue 1, pages 142-9, Jan 2008, PMID 18175748
- ↑ M. Ristow, K. Zarse, A. Oberbach, N. Kloting, M. Birringer, M. Kiehntopf, M. Stumvoll, C. R. Kahn, M. Bluher, Antioxidants prevent health-promoting effects of physical exercise in humans, Proceedings of the National Academy of Sciences, volume 106, issue 21, 2009, pages 8665–8670, ISSN 0027-8424, doi 10.1073/pnas.0903485106
- ↑ NA. Strobel, JM. Peake, A. Matsumoto, SA. Marsh, JS. Coombes, GD. Wadley, Antioxidant supplementation reduces skeletal muscle mitochondrial biogenesis., Med Sci Sports Exerc, volume 43, issue 6, pages 1017-24, Jun 2011, doi 10.1249/MSS.0b013e318203afa3, PMID 21085043
- ↑ GD. Wadley, GK. McConell, High-dose antioxidant vitamin C supplementation does not prevent acute exercise-induced increases in markers of skeletal muscle mitochondrial biogenesis in rats., J Appl Physiol, volume 108, issue 6, pages 1719-26, Jun 2010, doi 10.1152/japplphysiol.00127.2010, PMID 20395544
- ↑ K. Higashida, SH. Kim, M. Higuchi, JO. Holloszy, DH. Han, Normal adaptations to exercise despite protection against oxidative stress., Am J Physiol Endocrinol Metab, volume 301, issue 5, pages E779-84, Nov 2011, doi 10.1152/ajpendo.00655.2010, PMID 21750271
- ↑ Christina Yfanti, Thorbjörn Åkerström, Søren Nielsen, Anders R Nielsen, Remi Mounier, Ole H Mortensen, Jens Lykkesfeldt, Adam J Rose, Christian P Fischer, Bente K Pedersen, Antioxidant Supplementation Does Not Alter Endurance Training Adaptation, Medicine & Science in Sports & Exercise, 2009, pages 1, ISSN 0195-9131, doi 10.1249/MSS.0b013e3181cd76be
- ↑ Mayur K Ranchordas, David Rogerson, Hora Soltani, Joseph T Costello, Antioxidants for preventing and reducing muscle soreness after exercise: a Cochrane systematic review, British Journal of Sports Medicine, 2018, pages bjsports-2018-099599, ISSN 0306-3674, doi 10.1136/bjsports-2018-099599
- ↑ SC. Bryer, AH. Goldfarb, Effect of high dose vitamin C supplementation on muscle soreness, damage, function, and oxidative stress to eccentric exercise., Int J Sport Nutr Exerc Metab, volume 16, issue 3, pages 270-80, Jun 2006, PMID 16948483
- ↑ M. Kaminski, R. Boal, An effect of ascorbic acid on delayed-onset muscle soreness., Pain, volume 50, issue 3, pages 317-21, Sep 1992, PMID 1280803
- ↑ D. Thompson, C. Williams, SJ. McGregor, CW. Nicholas, F. McArdle, MJ. Jackson, JR. Powell, Prolonged vitamin C supplementation and recovery from demanding exercise., Int J Sport Nutr Exerc Metab, volume 11, issue 4, pages 466-81, Dec 2001, PMID 11915781
- ↑ DA. Connolly, C. Lauzon, J. Agnew, M. Dunn, B. Reed, The effects of vitamin C supplementation on symptoms of delayed onset muscle soreness., J Sports Med Phys Fitness, volume 46, issue 3, pages 462-7, Sep 2006, PMID 16998453
- ↑ Graeme L. Close, Tony Ashton, Tim Cable, Dominic Doran, Chris Holloway, Frank McArdle, Don P. M. MacLaren, Ascorbic acid supplementation does not attenuate post-exercise muscle soreness following muscle-damaging exercise but may delay the recovery process, British Journal of Nutrition, volume 95, issue 5, 2006, pages 976–981, ISSN 00071145, doi 10.1079/BJN20061732
- ↑ D. Thompson, C. Williams, M. Kingsley, CW. Nicholas, HK. Lakomy, F. McArdle, MJ. Jackson, Muscle soreness and damage parameters after prolonged intermittent shuttle-running following acute vitamin C supplementation., Int J Sports Med, volume 22, issue 1, pages 68-75, Jan 2001, doi 10.1055/s-2001-11358, PMID 11258644
- ↑ D. Thompson, DM. Bailey, J. Hill, T. Hurst, JR. Powell, C. Williams, Prolonged vitamin C supplementation and recovery from eccentric exercise., Eur J Appl Physiol, volume 92, issue 1-2, pages 133-8, Jun 2004, doi 10.1007/s00421-004-1064-y, PMID 15024666
- ↑ LJ. Beaton, DA. Allan, MA. Tarnopolsky, PM. Tiidus, SM. Phillips, Contraction-induced muscle damage is unaffected by vitamin E supplementation., Med Sci Sports Exerc, volume 34, issue 5, pages 798-805, May 2002, PMID 11984298
- ↑ A. Shafat, P. Butler, RL. Jensen, AE. Donnelly, Effects of dietary supplementation with vitamins C and E on muscle function during and after eccentric contractions in humans., Eur J Appl Physiol, volume 93, issue 1-2, pages 196-202, Oct 2004, doi 10.1007/s00421-004-1198-y, PMID 15309547
- ↑ A. Mastaloudis, MG. Traber, K. Carstensen, JJ. Widrick, Antioxidants did not prevent muscle damage in response to an ultramarathon run., Med Sci Sports Exerc, volume 38, issue 1, pages 72-80, Jan 2006, PMID 16394956
- ↑ DM. High, ET. Howley, BD. Franks, The effects of static stretching and warm-up on prevention of delayed-onset muscle soreness., Res Q Exerc Sport, volume 60, issue 4, pages 357-61, Dec 1989, PMID 2489863
- ↑ 120.0 120.1 PH. Johansson, L. Lindström, G. Sundelin, B. Lindström, The effects of preexercise stretching on muscular soreness, tenderness and force loss following heavy eccentric exercise., Scand J Med Sci Sports, volume 9, issue 4, pages 219-25, Aug 1999, PMID 10407930
- ↑ Wessel, Jean, and Aaron Wan. "Effect of stretching on the intensity of delayed-onset muscle soreness." Clinical Journal of Sport Medicine 4.2 (1994): 83-87.
- ↑ Does Postexercise Static Stretching Alleviate Delayed Muscle Soreness? http://www.eric.ed.gov/ERICWebPortal/search/detailmini.jsp?_nfpb=true&_&ERICExtSearch_SearchValue_0=EJ414210&ERICExtSearch_SearchType_0=no&accno=EJ414210
- ↑ RD. Herbert, M. de Noronha, Stretching to prevent or reduce muscle soreness after exercise., Cochrane Database Syst Rev, issue 4, pages CD004577, 2007, doi 10.1002/14651858.CD004577.pub2, PMID 17943822
- ↑ H. Lund, P. Vestergaard-Poulsen, IL. Kanstrup, P. Sejrsen, The effect of passive stretching on delayed onset muscle soreness, and other detrimental effects following eccentric exercise., Scand J Med Sci Sports, volume 8, issue 4, pages 216-21, Aug 1998, PMID 9764443
- ↑ LL. Smith, MH. Brunetz, TC. Chenier, MR. McCammon, JA. Houmard, ME. Franklin, RG. Israel, The effects of static and ballistic stretching on delayed onset muscle soreness and creatine kinase., Res Q Exerc Sport, volume 64, issue 1, pages 103-7, Mar 1993, PMID 8451526
- ↑ Yanfei Xie, Beibei Feng, Kedi Chen, Lars L. Andersen, Phil Page, Yuling Wang, The Efficacy of Dynamic Contract-Relax Stretching on Delayed-Onset Muscle Soreness Among Healthy Individuals, Clinical Journal of Sport Medicine, volume 28, issue 1, 2018, pages 28–36, ISSN 1050-642X, doi 10.1097/JSM.0000000000000442
- ↑ DK. Mishra, J. Fridén, MC. Schmitz, RL. Lieber, Anti-inflammatory medication after muscle injury. A treatment resulting in short-term improvement but subsequent loss of muscle function., J Bone Joint Surg Am, volume 77, issue 10, pages 1510-9, Oct 1995, PMID 7593059
- ↑ R.S. Ramsewak, D.L. DeWitt, M.G. Nair, Cytotoxicity, antioxidant and anti-inflammatory activities of Curcumins I–III from Curcuma longa, Phytomedicine, volume 7, issue 4, 2000, pages 303–308, ISSN 09447113, doi 10.1016/S0944-7113(00)80048-3
- ↑ 129.0 129.1 LM. Nicol, DS. Rowlands, R. Fazakerly, J. Kellett, Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS)., Eur J Appl Physiol, volume 115, issue 8, pages 1769-77, Aug 2015, doi 10.1007/s00421-015-3152-6, PMID 25795285
- ↑ 130.0 130.1 F. Drobnic, J. Riera, G. Appendino, S. Togni, F. Franceschi, X. Valle, A. Pons, J. Tur, Reduction of delayed onset muscle soreness by a novel curcumin delivery system (Meriva): a randomised, placebo-controlled trial., J Int Soc Sports Nutr, volume 11, pages 31, 2014, doi 10.1186/1550-2783-11-31, PMID 24982601
- ↑ 131.0 131.1 Lesley M. Nicol, David S. Rowlands, Ruth Fazakerly, John Kellett, Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS), European Journal of Applied Physiology, volume 115, issue 8, 2015, pages 1769–1777, ISSN 1439-6319, doi 10.1007/s00421-015-3152-6
- ↑ 132.0 132.1 132.2 Brian K. McFarlin, Adam S. Venable, Andrea L. Henning, Jill N. Best Sampson, Kathryn Pennel, Jakob L. Vingren, David W. Hill, Reduced Inflammatory and Muscle Damage Biomarkers following Oral Supplementation with Bioavailable Curcumin, BBA Clinical, 2016, ISSN 22146474, doi 10.1016/j.bbacli.2016.02.003
- ↑ 133.0 133.1 133.2 133.3 133.4 Yoko Tanabe, Seiji Maeda, Nobuhiko Akazawa, Asako Zempo-Miyaki, Youngju Choi, Song-Gyu Ra, Atsushi Imaizumi, Yoshihiko Otsuka, Kazunori Nosaka, Attenuation of indirect markers of eccentric exercise-induced muscle damage by curcumin, European Journal of Applied Physiology, volume 115, issue 9, 2015, pages 1949–1957, ISSN 1439-6319, doi 10.1007/s00421-015-3170-4
- ↑ 134.0 134.1 134.2 JM. Davis, EA. Murphy, MD. Carmichael, MR. Zielinski, CM. Groschwitz, AS. Brown, JD. Gangemi, A. Ghaffar, EP. Mayer, Curcumin effects on inflammation and performance recovery following eccentric exercise-induced muscle damage., Am J Physiol Regul Integr Comp Physiol, volume 292, issue 6, pages R2168-73, Jun 2007, doi 10.1152/ajpregu.00858.2006, PMID 17332159
- ↑ N. Kawanishi, K. Kato, M. Takahashi, T. Mizokami, Y. Otsuka, A. Imaizumi, D. Shiva, H. Yano, K. Suzuki, Curcumin attenuates oxidative stress following downhill running-induced muscle damage., Biochem Biophys Res Commun, volume 441, issue 3, pages 573-8, Nov 2013, doi 10.1016/j.bbrc.2013.10.119, PMID 24184481
- ↑ 136.0 136.1 SM. Hasson, JC. Daniels, JG. Divine, BR. Niebuhr, S. Richmond, PG. Stein, JH. Williams, Effect of ibuprofen use on muscle soreness, damage, and performance: a preliminary investigation., Med Sci Sports Exerc, volume 25, issue 1, pages 9-17, Jan 1993, PMID 8423760
- ↑ 137.0 137.1 author Tokmakidis SP, Kokkinidis EA, Smilios I, Douda H, The effects of ibuprofen on delayed muscle soreness and muscular performance after eccentric exercise., J Strength Cond Res, 2003, volume 17, issue 1, pages 53-9, PMID 12580656
- ↑ 138.0 138.1 Effect of Ibuprofen Use on Delayed Onset Muscle Soreness of the Elbow Flexors http://journals.humankinetics.com/jsr-back-issues/jsrvolume4issue4november/effectofibuprofenuseondelayedonsetmusclesorenessoftheelbowflexors
- ↑ 139.0 139.1 FX. Pizza, D. Cavender, A. Stockard, H. Baylies, A. Beighle, Anti-inflammatory doses of ibuprofen: effect on neutrophils and exercise-induced muscle injury., Int J Sports Med, volume 20, issue 2, pages 98-102, Feb 1999, doi 10.1055/s-2007-971100, PMID 10190769
- ↑ 140.0 140.1 Joel R. Krentz, Braden Quest, Jonathan P. Farthing, Dale W. Quest, Philip D. Chilibeck, The effects of ibuprofen on muscle hypertrophy, strength, and soreness during resistance training, Applied Physiology, Nutrition, and Metabolism, volume 33, issue 3, 2008, pages 470–475, ISSN 1715-5312, doi 10.1139/H08-019
- ↑ 141.0 141.1 Lars Arendt-Nielsen, Morten Weidner, Dorte Bartholin, Allan Rosetzsky, A Double-Blind Randomized Placebo Controlled Parallel Group Study Evaluating the Effects of Ibuprofen and Glucosamine Sulfate on Exercise Induced Muscle Soreness, Journal Of Musculoskeletal Pain, volume 15, issue 1, 2007, pages 21–28, ISSN 1058-2452, doi 10.1300/J094v15n01_04
- ↑ 142.0 142.1 AE. Donnelly, RJ. Maughan, PH. Whiting, Effects of ibuprofen on exercise-induced muscle soreness and indices of muscle damage., Br J Sports Med, volume 24, issue 3, pages 191-5, Sep 1990, PMID 2078806
- ↑ 143.0 143.1 143.2 MB. Stone, MA. Merrick, CD. Ingersoll, JE. Edwards, Preliminary comparison of bromelain and Ibuprofen for delayed onset muscle soreness management., Clin J Sport Med, volume 12, issue 6, pages 373-8, Nov 2002, PMID 12466693
- ↑ Robert D. Hyldahl, Justin Keadle, Pierre A. Rouzier, Dennis Pearl, Priscilla M. Clarkson, Effects of Ibuprofen Topical Gel on Muscle Soreness, Medicine & Science in Sports & Exercise, volume 42, issue 3, 2010, pages 614–621, ISSN 0195-9131, doi 10.1249/MSS.0b013e3181b95db2
- ↑ 145.0 145.1 145.2 P. Barlas, JA. Craig, J. Robinson, DM. Walsh, GD. Baxter, JM. Allen, Managing delayed-onset muscle soreness: lack of effect of selected oral systemic analgesics., Arch Phys Med Rehabil, volume 81, issue 7, pages 966-72, Jul 2000, doi 10.1053/apmr.2000.6277, PMID 10896014
- ↑ 146.0 146.1 Lucille Smith, Robert George, Thomas Chenier, Michael McCammon, Joseph Houmard, Richard Israel, R. A. Hoppmann, Susan Smith, Do over-the-counter analgesics reduce delayed onset muscle soreness and serum creatine kinase values?, Research in Sports Medicine, volume 6, issue 2, 1995, pages 81–88, ISSN 1543-8627, doi 10.1080/15438629509512039
- ↑ 147.0 147.1 Riasati et al.: Aspirin and delayed onset muscle soreness ASPIRIN MAY BE AN EFFECTIVE TREATMENT FOR EXERCISE- INDUCED MUSCLE SORENESS | ResearchGate http://www.researchgate.net/publication/228091056_Riasati_et_al._Aspirin_and_delayed_onset_muscle_soreness_ASPIRIN_MAY_BE_AN_EFFECTIVE_TREATMENT_FOR_EXERCISE-_INDUCED_MUSCLE_SORENESS
- ↑ 148.0 148.1 KT. Francis, T. Hoobler, Effects of aspirin on delayed muscle soreness., J Sports Med Phys Fitness, volume 27, issue 3, pages 333-7, Sep 1987, PMID 3431117
- ↑ 149.0 149.1 GA. Dudley, J. Czerkawski, A. Meinrod, G. Gillis, A. Baldwin, M. Scarpone, Efficacy of naproxen sodium for exercise-induced dysfunction muscle injury and soreness., Clin J Sport Med, volume 7, issue 1, pages 3-10, Jan 1997, PMID 9117523
- ↑ 150.0 150.1 AC. Baldwin, SW. Stevenson, GA. Dudley, Nonsteroidal anti-inflammatory therapy after eccentric exercise in healthy older individuals., J Gerontol A Biol Sci Med Sci, volume 56, issue 8, pages M510-3, Aug 2001, PMID 11487604
- ↑ 151.0 151.1 JM. Lecomte, VJ. Lacroix, DL. Montgomery, A randomized controlled trial of the effect of naproxen on delayed onset muscle soreness and muscle strength., Clin J Sport Med, volume 8, issue 2, pages 82-7, Apr 1998, PMID 9641434
- ↑ The Effect of Taking Naproxen Drug on the Level of Perceived Pain and Changes of CPK Serum after Eccentric Exercise - Harakat Volume: 37, Issue:, Accessed on 3 January 2013
- ↑ 153.0 153.1 J. Bourgeois, D. MacDougall, J. MacDonald, M. Tarnopolsky, Naproxen does not alter indices of muscle damage in resistance-exercise trained men., Med Sci Sports Exerc, volume 31, issue 1, pages 4-9, Jan 1999, PMID 9927002
- ↑ A E Donnelly, K McCormick, R J Maughan, P H Whiting, P M Clarkson, Effects of a non-steroidal anti-inflammatory drug on delayed onset muscle soreness and indices of damage., British Journal of Sports Medicine, volume 22, issue 1, 1988, pages 35–38, ISSN 0306-3674, doi 10.1136/bjsm.22.1.35
- ↑ L.C. Loram, D. Mitchell, A. Fuller, Rofecoxib and tramadol do not attenuate delayed-onset muscle soreness or ischaemic pain in human volunteers, Canadian Journal of Physiology and Pharmacology, volume 83, issue 12, 2005, pages 1137–1145, ISSN 0008-4212, doi 10.1139/y05-113
- ↑ 156.0 156.1 SP. Sayers, CA. Knight, PM. Clarkson, EH. Van Wegen, G. Kamen, Effect of ketoprofen on muscle function and sEMG activity after eccentric exercise., Med Sci Sports Exerc, volume 33, issue 5, pages 702-10, May 2001, PMID 11323536
- ↑ Morgan E. Chaffin, Kris E. Berg, Jessica R. Meendering, Tamra L. Llewellyn, Jeffrey A. French, Jeremy E. Davis, Interleukin-6 and Delayed Onset Muscle Soreness Do Not Vary During the Menstrual Cycle, Research Quarterly for Exercise and Sport, volume 82, issue 4, 2011, pages 693–701, ISSN 0270-1367, doi 10.1080/02701367.2011.10599806
- ↑ J Schwane, Is lactic acid related to delayed-onset muscle soreness., Physician & Sportsmedicin, volume 11, issue 3, pages 124-127;130-131, Mar 1983
- ↑ MP. McHugh, Recent advances in the understanding of the repeated bout effect: the protective effect against muscle damage from a single bout of eccentric exercise., Scand J Med Sci Sports, volume 13, issue 2, pages 88-97, Apr 2003, PMID 12641640
- ↑ MP. McHugh, DA. Connolly, RG. Eston, GW. Gleim, Exercise-induced muscle damage and potential mechanisms for the repeated bout effect., Sports Med, volume 27, issue 3, pages 157-70, Mar 1999, PMID 10222539
- ↑ R. Lynn, JA. Talbot, DL. Morgan, Differences in rat skeletal muscles after incline and decline running., J Appl Physiol (1985), volume 85, issue 1, pages 98-104, Jul 1998, PMID 9655761
- Category:Pages with reference errors